
The relationship of lung recruitability assessment by recruitment to inflation ratio, electrical impedance tomography, and lung ultrasound: The research protocol
Recruitability assessment method by bedside imaging tools
DOI:
https://doi.org/10.54205/ccc.v31.260228Keywords:
Acute respiratory distress syndrome, Recruitment-to-inflation ratio, Lung ultrasonography, Electrical impedance tomography, Recruitability assessmentAbstract
Background: Recently, the recruitment-to-inflation ratio (R/I ratio) from the single-breath technique has been proposed for identifying lung recruitability in acute respiratory distress syndrome (ARDS). This technique is based on measuring end-expiratory lung volume (EELV). Also, electrical impedance tomography (EIT) can estimate the EELV, providing the potential role of EIT in measuring the R/I ratio. In addition, the lung ultrasound was proved to identify lung recruitment. However, a study validating those techniques has not been conducted.
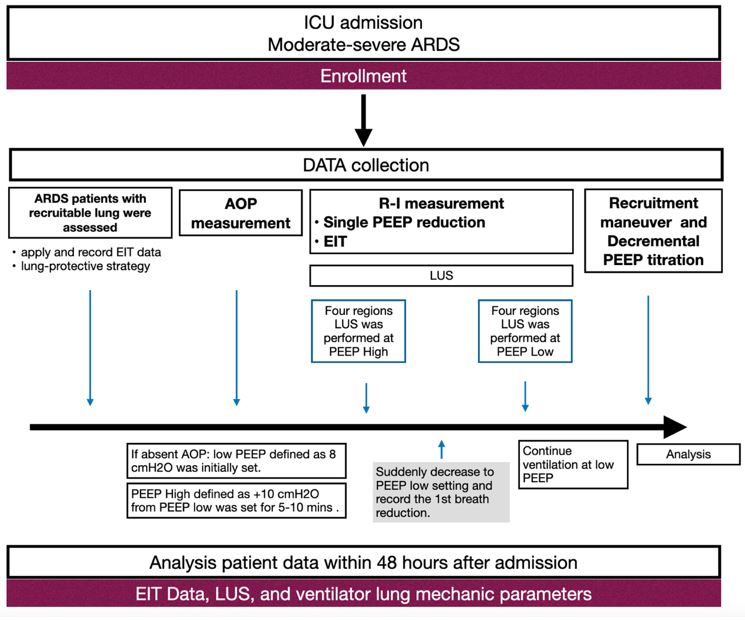
Methods: We plan to conduct a single-center prospective physiological study on moderate to severe ARDS patients. The R/I ratio by single-breath technique and EIT will be collected before the recruitment maneuver. If the patient has no airway opening pressure (AOP), PEEP of 8 cmH2O will be set as PEEPlow. The PEEPhigh defines as initially set at +10 cmH2O from the PEEPlow. However, if the patients have AOP presence, AOP +10 cmH2O will be set as PEEPhigh The lung ultrasound score (LUS) will be performed at PEEPhigh and PEEPlow during the single-breath technique. Variables that will be used to analyze the relationship are recruited volume (Vrec), R/I ratio, and LUS.
Hypothesis: We hypothesize that there are associations between the R/I ratio by both techniques and lung ultrasound score (LUS).
Ethics: The study protocol has been approved by the ethics committee of the faculty of medicine, Ramathibodi Hospital, Mahidol University (COA.MURA2021/433).
Downloads
References
Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526-33.
Malbouisson LM, Muller JC, Constantin JM, Lu Q, Puybasset L, Rouby JJ, et al. Computed tomography assessment of positive end-expiratory pressure-induced alveolar recruitment in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001;163:1444-50.
Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, et al. Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med. 2006;354:1775-86.
Puybasset L, Cluzel P, Chao N, Slutsky AS, Coriat P, Rouby JJ. A computed tomography scan assessment of regional lung volume in acute lung injury. The CT Scan ARDS Study Group. Am J Respir Crit Care Med. 1998;158:1644-55.
Caironi P, Cressoni M, Chiumello D, Ranieri M, Quintel M, Russo SG, et al. Lung opening and closing during ventilation of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2010;181:578-86.
Chiumello D, Marino A, Brioni M, Cigada I, Menga F, Colombo A, et al. Lung recruitment assessed by respiratory mechanics and computed tomography in patients with acute respiratory distress syndrome. What is the relationship? Am J Respir Crit Care Med. 2016;193:1254-63.
Demory D, Arnal JM, Wysocki M, Donati S, Granier I, Corno G, et al. Recruitability of the lung estimated by the pressure volume curve hysteresis in ARDS patients. Intensive Care Med. 2008;34:2019-25.
Dellamonica J, Lerolle N, Sargentini C, Beduneau G, Di Marco F, Mercat A, et al. Accuracy and precision of end-expiratory lung-volume measurements by automated nitrogen washout/washin technique in patients with acute respiratory distress syndrome. Crit Care. 2011;15:R294.
Chen L, Del Sorbo L, Grieco DL, Junhasavasdikul D, Rittayamai N, Soliman I, et al. Potential for lung recruitment estimated by the recruitment-to-inflation ratio in acute respiratory distress syndrome. A Clinical Trial. Am J Respir Crit Care Med. 2020;201:178-87.
Bouhemad B, Brisson H, Le-Guen M, Arbelot C, Lu Q, Rouby JJ. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am J Respir Crit Care Med. 2011;183:341-7.
Yun L, He HW, Moller K, Frerichs I, Liu D, Zhao Z. Assessment of lung recruitment by electrical impedance tomography and oxygenation in ARDS patients. Medicine (Baltimore). 2016;95:e3820.
Global initiative for chronic obstructive lung disease, Global strategy for diagnosis, management and prevention of COPD 2022 update. 2022.
Akoumianaki E, Maggiore SM, Valenza F, Bellani G, Jubran A, Loring SH, et al. The application of esophageal pressure measurement in patients with respiratory failure. Am J Respir Crit Care Med. 2014;189:520-31.
Baedorf Kassis E, Loring SH, Talmor D. Mortality and pulmonary mechanics in relation to respiratory system and transpulmonary driving pressures in ARDS. Intensive Care Med. 2016;42:1206-13.
Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010;303:865-73.
Kacmarek RM, Villar J, Sulemanji D, Montiel R, Ferrando C, Blanco J, et al. Open lung approach for the acute respiratory distress syndrome: A pilot, randomized controlled trial. Crit Care Med. 2016;44:32-42.
Writing group for the alveolar recruitment for acute respiratory distress syndrome trial I, Cavalcanti AB, Suzumura EA, Laranjeira LN, Paisani DM, Damiani LP, et al. Effect of lung recruitment and titrated Positive End-Expiratory Pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA. 2017;318:1335-45.
Hodgson CL, Cooper DJ, Arabi Y, King V, Bersten A, Bihari S, et al. Maximal recruitment open lung ventilation in acute respiratory distress syndrome (PHARLAP). A phase II, multicenter randomized controlled clinical trial. Am J Respir Crit Care Med. 2019;200:1363-72.
Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. Lung ultrasound for critically ill patients. Am J Respir Crit Care Med. 2019;199:701-14.
Karsten J, Meier T, Iblher P, Schindler A, Paarmann H, Heinze H. The suitability of EIT to estimate EELV in a clinical trial compared to oxygen wash-in/wash-out technique. Biomed Tech (Berl). 2014;59:59-64.
Mauri T, Eronia N, Turrini C, Battistini M, Grasselli G, Rona R, et al. Bedside assessment of the effects of positive end-expiratory pressure on lung inflation and recruitment by the helium dilution technique and electrical impedance tomography. Intensive Care Med. 2016;42:1576-87.
Wang YM, Sun XM, Zhou YM, Chen JR, Cheng KM, Li HL, et al. Use of electrical impedance tomography (EIT) to estimate global and regional lung recruitment volume (VREC) induced by positive end-expiratory pressure (PEEP): An experiment in pigs with lung injury. Med Sci Monit. 2020;26:e922609.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2023 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

