
Change in cardiac index during Trendelenburg maneuver as a predictor of fluid responsiveness among patients under mechanical ventilation with spontaneous breathing activity: A protocol for prospective observational study
Trendelenburg maneuver and fluid responsiveness in mechanically ventilated patients with spontaneous breathing activity
DOI:
https://doi.org/10.54205/ccc.v32.266258Keywords:
Trendelenburg maneuver, Fluid responsiveness, Spontaneous breathing activity, Cardiac indexAbstract
Background: Optimal fluid management in surgical intensive care units (SICUs) is challenging, with under or over-resuscitations linked to increased mortality and extended ICU stays. Dynamic parameters like stroke volume variation and pulse pressure variation are unreliable in intubated patients with spontaneous breathing activity. The passive leg raise (PLR), which relies on translocation of the patient’s intravascular volume, is effective in identifying fluid responsiveness, but it still has some limitations. Regarding limitations, another potential method, using the same principle, known as the Trendelenburg maneuver (TM), has been introduced. This study aims to assess the diagnostic performance of TM in mechanically ventilated patients with spontaneous breathing activity, focusing on changes in cardiac index in relation to fluid administration.
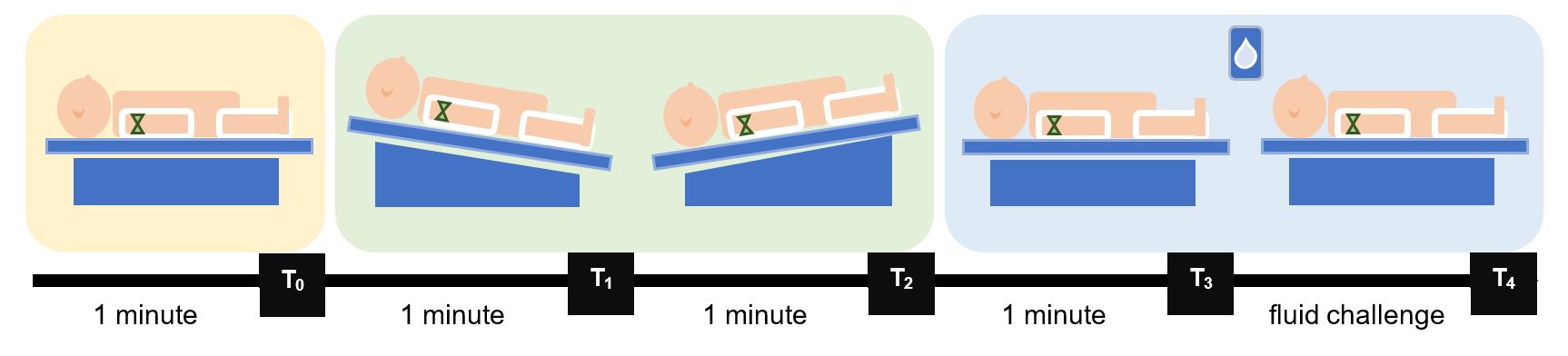
Methods: In this single-center, prospective observational study conducted in a surgical ICU, we enrolled 68 patients with inadequate tissue perfusion who had spontaneous breathing while receiving mechanical ventilation to evaluate the diagnostic ability of TM in fluid responsiveness prediction. The patients were classified as fluid responders when the change in cardiac index, measured by the FloTrac™ sensor with the HemoSphere™ advanced monitoring platform, increased by more than 10% after fluid administration.
Hypothesis: We hypothesize that TM has the ability to predict fluid responsiveness in mechanically ventilated patients with spontaneous breathing activity.
Ethics and dissemination: This trial received approval from the Siriraj Institutional Review Board. We plan to present the result in peer-reviewed publications in critical care medicine.
Trial registration: TCTR20230704005
Downloads
References
Shen Y, Huang X, Zhang W. Association between fluid intake and mortality in critically ill patients with negative fluid balance: a retrospective cohort study. Crit Care. 2017;21:104.
Lee J, de Louw E, Niemi M, Nelson R, Mark RG, Celi LA, et al. Association between fluid balance and survival in critically ill patients. J Intern Med. 2015;277:468-77.
Koonrangsesomboon W, Khwannimit B. Impact of positive fluid balance on mortality and length of stay in septic shock patients. Indian J Crit Care Med. 2015;19:708-13.
Yonis H, Bitker L, Aublanc M, Perinel Ragey S, Riad Z, Lissonde F, et al. Change in cardiac output during Trendelenburg maneuver is a reliable predictor of fluid responsiveness in patients with acute respiratory distress syndrome in the prone position under protective ventilation. Crit Care. 2017;21:295.
Luo JC, Su Y, Dong LL, Hou JY, Li X, Zhang Y, et al. Trendelenburg maneuver predicts fluid responsiveness in patients on veno-arterial extracorporeal membrane oxygenation. Ann Intensive Care. 2021;11:16.
Bednarczyk JM, Fridfinnson JA, Kumar A, Blanchard L, Rabbani R, Bell D, et al. Incorporating dynamic assessment of fluid responsiveness into goal-directed therapy: A systematic review and meta-analysis. Crit Care Med. 2017;45:1538-45.
Monnet X, Rienzo M, Osman D, Anguel N, Richard C, Pinsky MR, et al. Passive leg raising predicts fluid responsiveness in the critically ill. Crit Care Med. 2006;34:1402-7.
Magder S. Clinical usefulness of respiratory variations in arterial pressure. Am J Respir Crit Care Med. 2004;169:151-5.
Chaves RCF, Correa TD, Neto AS, Bravim BA, Cordioli RL, Moreira FT, et al. Assessment of fluid responsiveness in spontaneously breathing patients: a systematic review of literature. Ann Intensive Care. 2018;8:21.
Monnet X, Marik P, Teboul JL. Passive leg raising for predicting fluid responsiveness: a systematic review and meta-analysis. Intensive Care Med. 2016;42:1935-47.
Cavallaro F, Sandroni C, Marano C, La Torre G, Mannocci A, De Waure C, et al. Diagnostic accuracy of passive leg raising for prediction of fluid responsiveness in adults: systematic review and meta-analysis of clinical studies. Intensive Care Med. 2010;36:1475-83.
Min JH, Lee SE, Lee HS, Chae YK, Lee YK, Kang Y, et al. The correlation between the Trendelenburg position and the stroke volume variation. Korean J Anesthesiol. 2014;67:378-83.
Terai C, Anada H, Matsushima S, Kawakami M, Okada Y. Effects of Trendelenburg versus passive leg raising: autotransfusion in humans. Intensive Care Med. 1996;22:613-4.
Toppen W, Aquije Montoya E, Ong S, Markovic D, Kao Y, Xu X, et al. Passive leg raise: Feasibility and safety of the maneuver in patients with undifferentiated shock. J Intensive Care Med. 2020;35:1123-8.
Monnet X, Teboul JL. Passive leg raising: five rules, not a drop of fluid! Crit Care. 2015;19:18.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

