
End expiratory occlusion test and tidal volume challenge test for assess fluid responsiveness in prone patients
End expiratory occlusion test in prone patient
DOI:
https://doi.org/10.54205/ccc.v33.269629Keywords:
Fluid responsiveness, Tidal volume challenge test, End expiratory occlusion test, Prone positionAbstract
Background: Assessing fluid responsiveness in patients in the prone position with low tidal volume ventilation presents challenges when utilizing pulse pressure variation (PPV) and the inferior vena cava (IVC) distensibility index. These challenges stem from the use of low tidal volume and the difficulty of conducting IVC assessment in the prone position. Consequently, an alternative method for predicting fluid responsiveness in these patients is imperative.
Method: This study comprises a prospective investigation that was carried out on hypotensive patients positioned in the prone posture and undergoing lung-protective ventilation at Bhumibol Adulyadej Hospital. Prior to the administration of a 500 ml fluid bolus, end-expiratory occlusion (EEO) and tidal volume challenge (TVC) tests were conducted. Initial recordings of cardiac output, cardiac index, and PPV were documented, followed by subsequent recordings after each procedure.
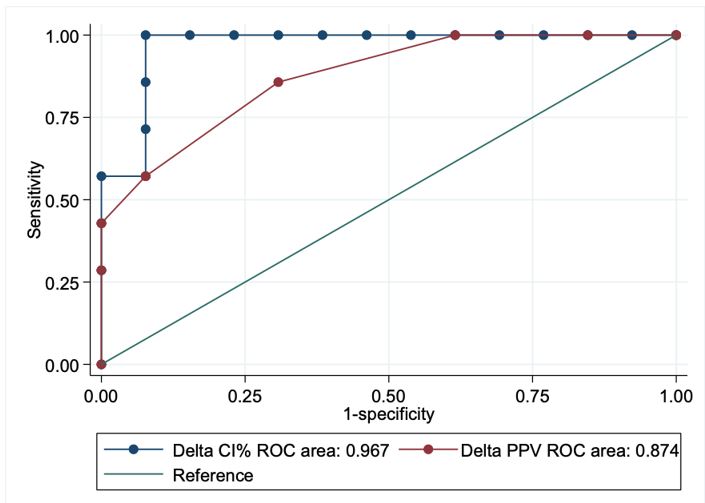
Result: Among the 20 participants in the prone position study, 4 patients developed severe acute respiratory distress syndrome (ARDS) while 16 patients were in that position for surgical reasons. Of these, 7 patients exhibited a positive response to fluid administration, while 13 patients did not. An increase in cardiac index (CI) of more than 5% during EEO is indicative of fluid responsiveness with a sensitivity of 100% and specificity of 92.3%. Moreover, a 3.5% absolute increment in PPV during TVC suggests fluid responsiveness with a sensitivity of 57.1% and specificity of 92.3%. We observed an interrater reliability (kappa) of 0.894 for EEO and 0.529 for PPV.
Conclusion: In the case of hypotensive patients undergoing prone positioning and receiving low tidal volume ventilation, both EEO for 15 seconds and TVC methodologies can be employed to evaluate fluid responsiveness. It is important to note that EEO demonstrates greater reliability in this context.
Downloads
References
Mikkelsen ME, Shah CV, Meyer NJ, Gaieski DF, Lyon S, Miltiades AN, et al. The epidemiology of acute respiratory distress syndrome in patients presenting to the emergency department with severe sepsis. Shock. 2013;40(5):375–81.
Qadir N, Sahetya S, Munshi L, Summers C, Abrams D, Beitler J, et al. An update on management of adult patients with acute respiratory distress syndrome: An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2024;209(1):24–36.
Gorman EA, O’Kane CM, McAuley DF. Acute respiratory distress syndrome in adults: diagnosis, outcomes, long-term sequelae, and management. The Lancet. 2022;400(10358):1157–70.
Shi R, Monnet X, Teboul JL. Parameters of fluid responsiveness: Current Opinion in Critical Care. 2020;26(3):319–26.
Marik PE, Monnet X, Teboul JL. Hemodynamic parameters to guide fluid therapy. 2011;9
De Backer D, Aissaoui N, Cecconi M, Chew MS, Denault A, Hajjar L, et al. How can assessing hemodynamics help to assess volume status? Intensive Care Med. 2022;48(10):1482–94
Gavelli F, Shi R, Teboul JL, Azzolina D, Monnet X. The end-expiratory occlusion test for detecting preload responsiveness: a systematic review and meta-analysis. Ann Intensive Care. 2020;10(1):65.
Gavelli F, Teboul JL, Monnet X. The end-expiratory occlusion test: please, let me hold your breath! Crit Care. 2019;23(1):274.
Messina A, Montagnini C, Cammarota G, Giuliani F, Muratore L, Baggiani M, et al. Assessment of fluid responsiveness in prone neurosurgical patients undergoing protective ventilation: Role of dynamic indices, tidal volume challenge, and end-expiratory occlusion test. Anesthesia & Analgesia. 2020;130(3):752–61.
Shi R, Ayed S, Moretto F, Azzolina D, De Vita N, Gavelli F, et al. Tidal volume challenge to predict preload responsiveness in patients with acute respiratory distress syndrome under prone position. Crit Care. 2022;26(1):219.
McGee WT, Horswell JL, Calderon J, Janvier G, Van Severen T, Van den Berghe G, et al. Validation of a continuous, arterial pressure-based cardiac output measurement: a multicenter, prospective clinical trial. Crit Care. 2007;11(5):R105.
Arya VK, Al-Moustadi W, Dutta V. Cardiac output monitoring – invasive and noninvasive. Current Opinion in Critical Care. 2022;28(3):340–7.
Hofer CK, Senn A, Weibel L, Zollinger A. Assessment of stroke volume variation for prediction of fluid responsiveness using the modified FloTracTM and PiCCOplusTM system. Crit Care. 2008;12(3):R82.
Alvarado Sánchez JI, Caicedo Ruiz JD, Diaztagle Fernández JJ, Amaya Zuñiga WF, Ospina-Tascón GA, Cruz Martínez LE. Predictors of fluid responsiveness in critically ill patients mechanically ventilated at low tidal volumes: systematic review and meta-analysis. Ann Intensive Care. 2021;11(1):28.
Messina A, Calabrò L, Pugliese L, Lulja A, Sopuch A, Rosalba D, et al. Fluid challenge in critically ill patients receiving haemodynamic monitoring: a systematic review and comparison of two decades. Crit Care. 2022;26(1):181.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

