
Effect of positive end-expiratory pressure on intracranial pressure in post cranial surgery using ultrasonic imaging measurement the optic nerve sheath diameter
Impact of PEEP on intracranial pressure post-cranial surgery via optic nerve sheath imaging
DOI:
https://doi.org/10.54205/ccc.v33.274777Keywords:
Positive end expiratory pressure, Intracranial pressure, Optic nerve sheath diameter, Post cranial surgeryAbstract
Background: While positive end-expiratory pressure (PEEP) is beneficial for oxygenation, it may potentially increase intracranial pressure (ICP): especially in post-cranial surgical patients. The optic nerve sheath diameter (ONSD) is the non-invasive method of ICP measurement. Our study focuses on the association between PEEP and intracranial pressure (ICP) in post-cranial surgery patients using optic nerve sheath diameter (ONSD) as a surrogate marker.
Method: A prospective non-randomized interventional study was conducted on post-cranial surgical patients who required mechanical ventilation with ages 16-80 years, initial PEEP at 5 mmH2O were included in this study. Patients with intracranial hypertension (defined as ICP 22 mmHg), a history of traumatic brain injury, or cardiopulmonary disease at enrollment were excluded from the study. ONSD measurement was performed at varying PEEP levels from 5 to 20 cmH2O.
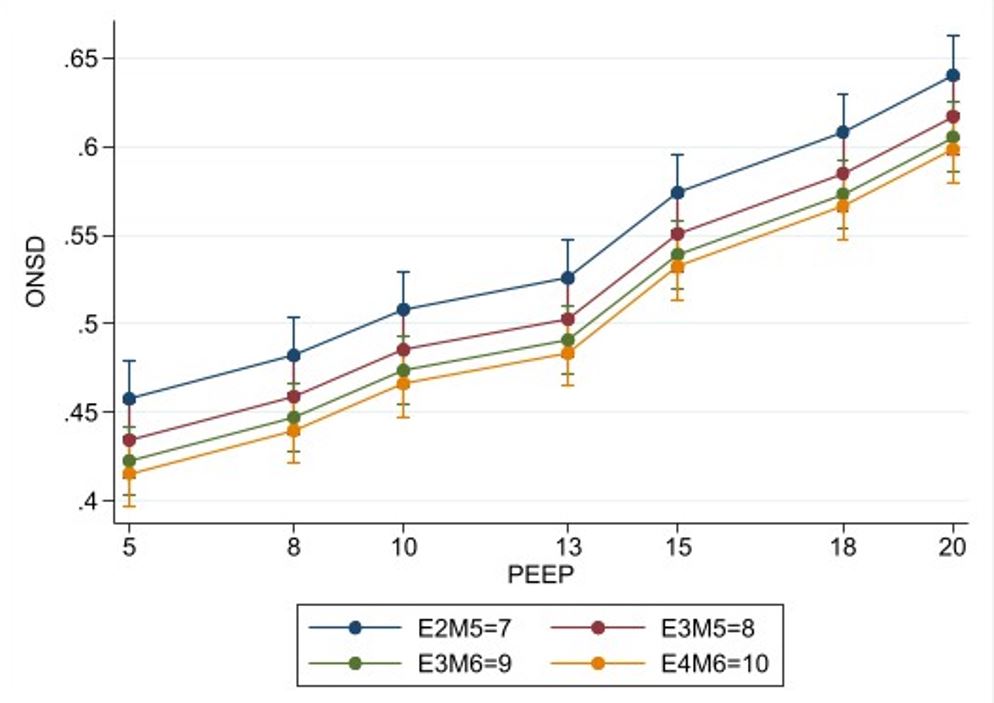
Result: In adult (18-60 years) patients who had post-cranial surgery within 72 hours and required a mechanical ventilator, ONSD corresponding to ICP significantly increased when PEEP exceeded 13 cmH2O. PEEP more than 15 cmH2O resulted in a significant increase in ONSD exceeding 5.5 mm (corresponding to ICP > 22 mmHg); Mean arterial pressure (MAP) significantly decreased with an increase in PEEP value (p < 0.001). PEEP 20 cmH2O reduced MAP to below 65 mmHg.
Conclusion: PEEP less than 15 cmH2O can be safely applied to post-cranial surgical patients, whereas PEEP more than 20 cmH2O may be harmful due to both ICP elevation and MAP decrement for these patients.
Downloads
References
González-Darder JM. History of the craniotomy. Neurocirugia (Astur). 2016;27(5):245-57.
Schizodimos T, Soulountsi V, Iasonidou C, Kapravelos N. An overview of management of intracranial hypertension in the intensive care unit. J Anesth. 2020;34(5):741-757.
Akins PT, Banerjee A, Guppy K, Silverthorn J, Fitzgibbon J, Nandan Y, et al. A 10-Year Analysis of 3693 Craniotomies during a transition to multidisciplinary teams, Protocols, and Pathways. Perm J. 2019; 23:18.209.
Nuttapon L, Anupharp P. An overview of neurosurgical division in Bhumibol Adulyadej Hospital. Basic training information for the inspection report WFME. 2020;2.
Balestreri M, Czosnyka M, Hutchinson P, Steiner LA, Hiler M, Smielewski P, et al. Impact of intracranial pressure and cerebral perfusion pressure on severe disability and mortality after head injury. Neurocrit Care. 2006;4(1):8-13.
Kirkman MA, Smith M. Intracranial pressure monitoring, cerebral perfusion pressure estimation, and ICP/CPP-guided therapy: a standard of care or optional extra after brain injury? BJA: British Journal of Anaesthesia. 2014;112(1):35-46.
Gupta DK, Bisht A, Batra P, Mathur P, Mahapatra AK. A cost effectiveness-based safety and efficacy study of resterilized intra-parenchymal catheter based intracranial pressure monitoring in developing world. Asian J Neurosurg. 2016;11(4):416-420.
Maissan IM, Dirven PJ, Haitsma IK, Hoeks SE, Gommers D, Stolker RJ. Ultrasonographic measured optic nerve sheath diameter as an accurate and quick monitor for changes in intracranial pressure. J Neurosurg. 2015;123(3):743-7.
Berhanu D, Ferreira JC, Abegão Pinto L, Aguiar de Sousa D, Lucas Neto L, Tavares Ferreira J. The role of optic nerve sheath ultrasonography in increased intracranial pressure: A systematic review and meta analysis. J Neurol Sci. 2023; 454:120853.
Lee K, Rincon F. Pulmonary complications in patients with severe brain injury. Crit Care Res Pract. 2012; 2012:207247.
Della Torre V, Badenes R, Corradi F, Racca F, Lavinio A, Matta B, et al. Acute respiratory distress syndrome in traumatic brain injury: how do we manage it? J Thorac Dis. 2017;9(12):5368-5381.
Gupta N, Singh VK, Jafa S. Correlation of positive end-expiratory and intracranial pressure using the ultrasonographic-guided measurement of optic nerve sheath diameter in traumatic brain injury patients. Neurol India. 2021;69(6):1670-1674.
Sekhon MS, McBeth P, Zou J, Qiao L, Kolmodin L, Henderson WR, et al. Association between optic nerve sheath diameter and mortality in patients with severe traumatic brain injury. Neurocrit Care. 2014;21(2):245-52.
Sorrentino E, Diedler J, Kasprowicz M, Budohoski KP, Haubrich C, Smielewski P, et al. Critical thresholds for cerebrovascular reactivity after traumatic brain injury. Neurocrit Care. 2012;16(2):258–66.
Robba C, Santori G, Czosnyka M, Corradi F, Bragazzi N, Padayachy L, et al. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2018;44(8):1284-1294.
Luzzi S, Elia A, Del Maestro M, Morotti A, Elbabaa SK, Cavallini A, et al. Timing, and surgical treatment of spontaneous intracerebral hemorrhage: systematic review and proposal of a management algorithm. World Neurosurg. 2019;124:e769-e778.
Riparbelli AC, Capion T, Møller K, Mathiesen TI, Olsen MH, Forsse A. Critical ICP thresholds in relation to outcome: Is 22 mmHg really the answer? Acta Neurochir (Wien). 2024;166(1):63.
Rosenthal G, Sanchez-Mejia RO, Phan N, Hemphill JC 3rd, Martin C, Manley GT. Incorporating a parenchymal thermal diffusion cerebral blood flow probe in bedside assessment of cerebral autoregulation and vasoreactivity in patients with severe traumatic brain injury. J Neurosurg. 114:62–70
Mahmood SS, Pinsky MR. Heart-lung interactions during mechanical ventilation: the basics. Ann Transl Med. 2018;6(18):349.
Shalendra S, PriyaT, DiwakarT, MayankD, Munish. Correlations of optic nerve sheath diameter with intracranial pressure, positive end-expiratory pressure and patient positioning in patients with severe traumatic brain injury on a mechanical ventilator in the ICU. Acta Intensive (Colom). 2025;13;165:63-69.
Robba C, Poole D, McNett M, Asehnoune K, Bösel J, Bruder N, et al. Mechanical ventilation in patients with acute brain injury: recommendations of the European Society of Intensive Care Medicine consensus. Intensive Care Med. 2020;46(12):2397-2410.
Greta Z, Denise B, Daniel AG. Management of mechanical ventilation in brain injury: hyperventilation and positive end-expiratory pressure. J Intensive Med. 2024r; 4(11):247-260
Chen H, Menon DK, Kavanagh BP. Impact of altered Airway pressure on intracranial pressure, perfusion, and oxygenation: a narrative review. Crit Care Med. 2019; 47:254–63.
Zhang XY, Yang ZJ, Wang QX, Fan HR. Impact of positive end-expiratory pressure on cerebral injury patients with hypoxemia. Am J Emerg Med. 2011;29(7):699-703.
Georgiadis D, Schwarz S, Baumgartner RW, Veltkamp R, Schwab S. Influence of positive end-expiratory pressure on intracranial pressure and cerebral perfusion pressure in patients with acute stroke. Stroke. 2001;32(9):2088-92.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

