
Passive head-up tilt for predicting fluid responsiveness in critically ill patients
Passive head-up tilt and fluid responsiveness
DOI:
https://doi.org/10.54205/ccc.v34.279538Keywords:
Fluid responsiveness, Fluid challenge test, Passive head-up tilt, Critical care, Intensive care unitAbstract
Background: Assessment of fluid responsiveness is crucial for optimizing hemodynamic management in critically ill patients. Conventional tests such as the passive leg-raising (PLR) maneuver or fluid challenge may be limited by equipment constraints. This study evaluated the ability of the passive head-up tilt (HUT) test to predict fluid responsiveness without external fluid loading or heart–lung interaction.
Method: This prospective observational study enrolled 52 critically ill adults with shock undergoing cardiac output monitoring using pulse contour analysis. Hemodynamic parameters, including systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), stroke volume (SV), and cardiac output (CO), were recorded at baseline, during a 45° head-up tilt, and after returning to the supine position. A standard fluid challenge (250 mL crystalloid or colloid over 15 minutes) was used as the reference, and fluid responsiveness was defined as a stroke volume increase of more than 10%. Diagnostic performance was analyzed using the area under the receiver operating characteristic (AUROC) curve.
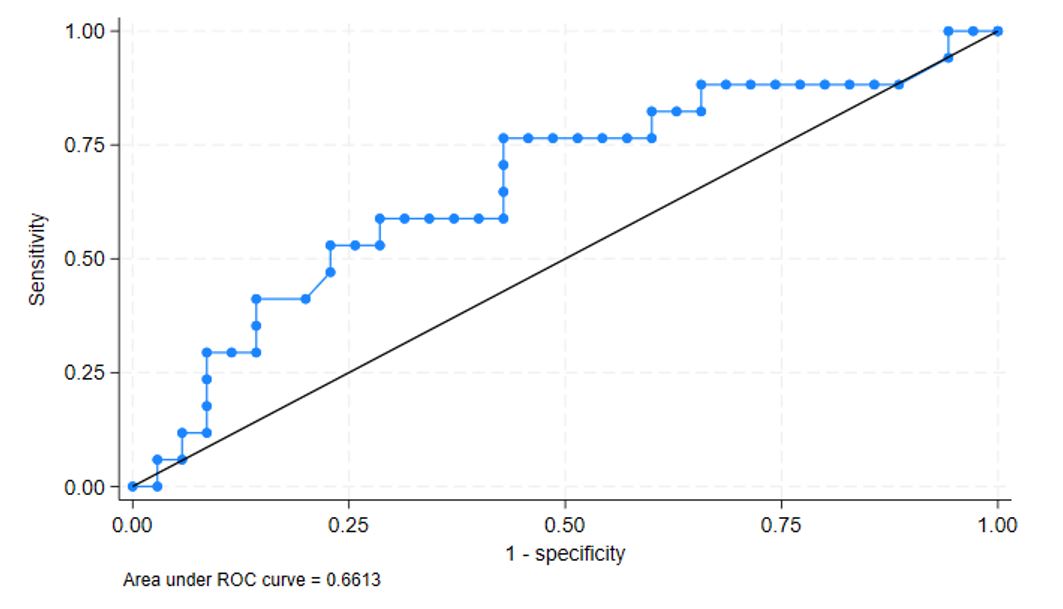
Result: Seventeen patients (32.7%) were responders. Most patients were in normal sinus rhythm (86.5%) and under positive-pressure ventilation (82.7%), with no between-group difference. The mean baseline CO was 4.8 L/min (IQR 3.75–6.4), and the mean SBP was 119.5 ± 17.6 mmHg. The change in SV from baseline to 1 minute after HUT showed the best diagnostic accuracy, with an AUROC = 0.67, sensitivity = 76%, and specificity = 57% at a 10% cutoff. Both SV and CO decreased during head elevation and increased after returning to supine, consistent with physiologic changes in venous return.
Conclusion: The passive head-up tilt test demonstrated poor to moderate accuracy for predicting fluid responsiveness. Rather than serving as a replacement for passive leg raising, HUT may be considered a supplementary or screening maneuver in situations where PLR is not feasible because of bed design or patient-related limitations.
Trial registration: TCTR20250129003
Downloads
References
Claure-Del Granado R, Mehta RL. Fluid overload in the ICU: evaluation and management. BMC Nephrol. 2016;17:109.
Malbrain MLNG, Nasa P, De Laet I, De Waele J, Jacobs R, Wise R, et al. Fluid Management in Intra-abdominal Hypertension. In: Malbrain MLNG, Wong A, Nasa P, Ghosh S, editors. Rational Use of Intravenous Fluids in Critically Ill Patients [Internet]. Cham: Springer International Publishing; 2024 [cited 2025 Dec 28]. p. 427–57. Available from: https://link.springer.com/10.1007/978-3-031-42205-8_22
Monnet X, Shi R, Teboul JL. Prediction of fluid responsiveness. What’s new? Ann Intensive Care. 2022;12:46.
Monnet X, Marik PE, Teboul JL. Prediction of fluid responsiveness: an update. Ann Intensive Care. 2016;6:111.
Monnet X, Teboul JL. Passive leg raising. Intensive Care Med. 2008;34:659–63.
Van Lieshout JJ, Harms MPM, Pott F, Jenstrup M, Secher NH. Stroke volume of the heart and thoracic fluid content during head‐up and head‐down tilt in humans. Acta Anaesthesiol Scand. 2005;49:1287–92.
Chaui-Berlinck JG, Monteiro LHA. Frank-Starling mechanism and short-term adjustment of cardiac flow. J Exp Biol. 2017;220:4391-4398.
O’Leary DD, Kimmerly DS, Cechetto AD, Shoemaker JK. Differential Effect of head‐up tilt on Cardiovagal and Sympathetic Baroreflex Sensitivity in Humans. Experimental Physiology. 2003;88:769–74.
Hajian-Tilaki K. Sample size estimation in diagnostic test studies of biomedical informatics. Journal of Biomedical Informatics. 2014;48:193–204.
Barthélémy R, Kindermans M, Delval P, Collet M, Gaugain S, Cecconi M, et al. Accuracy of cumulative volumes of fluid challenge to assess fluid responsiveness in critically ill patients with acute circulatory failure: a pharmacodynamic approach. British Journal of Anaesthesia. 2022;128:236–43.
Overall JE, Tonidandel S, Starbuck RR. Rule‐of‐thumb adjustment of sample sizes to accommodate dropouts in a two‐stage analysis of repeated measurements. Int J Methods Psych Res. 2006;15:1–11.
Messina A, Calabrò L, Pugliese L, Lulja A, Sopuch A, Rosalba D, et al. Fluid challenge in critically ill patients receiving haemodynamic monitoring: a systematic review and comparison of two decades. Crit Care. 2022;26:186.
AzuRea Group, Roger C, Zieleskiewicz L, Demattei C, Lakhal K, Piton G, et al. Time course of fluid responsiveness in sepsis: the fluid challenge revisiting (FCREV) study. Crit Care. 2019;23:179.
Youde J. Reproducibility of circulatory changes to head-up tilt in healthy elderly subjects. Age and Ageing. 2003;32:375–81.
Monnet X, Marik P, Teboul JL. Passive leg raising for predicting fluid responsiveness: a systematic review and meta-analysis. Intensive Care Med. 2016;42:1935–47.
Yonis H, Bitker L, Aublanc M, Perinel Ragey S, Riad Z, Lissonde F, et al. Change in cardiac output during Trendelenburg maneuver is a reliable predictor of fluid responsiveness in patients with acute respiratory distress syndrome in the prone position under protective ventilation. Crit Care. 2017;21:295.
Khwannimit B, Jomsuriya R. Comparison the accuracy and trending ability of cardiac index measured by the fourth-generation of FloTrac with the PiCCO device in septic shock patients. Turk J Med Sci. 2020;50(4):860–9.
Lima A, Klijn E, Bakker J, Ince C, Van Bommel J. Head-up tilt and passive leg raising in healthy volunteers as a preclinical model for preload-induced stroke volume modification. Crit Care. 2009;13:211.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

