
Phenotype-specific insulin strategies in shock states: A critical reappraisal
Phenotype-specific insulin in shock
DOI:
https://doi.org/10.54205/ccc.v34.279782Keywords:
Insulin, Septic shock, Cardiogenic shock, Septic cardiomyopathy, Metabolic resuscitation, High-dose insulin therapy, Glucose-Insulin-PotassiumAbstract
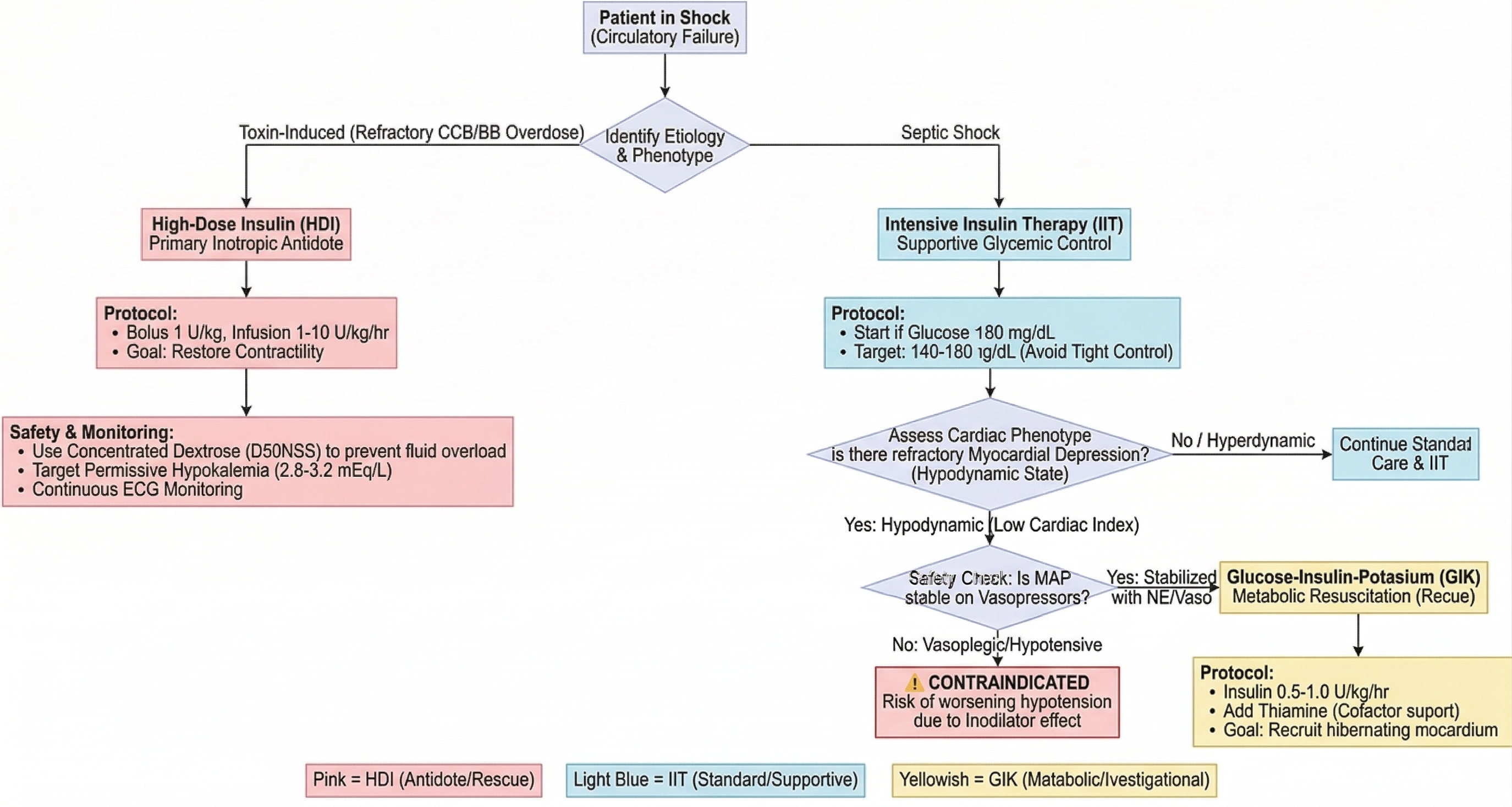
The use of insulin in critical care involves three distinct strategies: Intensive Insulin Therapy (IIT), High-Dose Insulin (HDI), and Glucose-Insulin-Potassium (GIK). This review clarifies their indications, mechanisms, and safety profiles. IIT primarily targets stress-induced hyperglycemia in sepsis; however, current guidelines recommend a moderate target (140–180 mg/dL) to avoid hypoglycemia, functioning as a supportive measure without direct mortality benefit. HDI serves as a potent inotropic antidote for refractory calcium channel blocker and beta-blocker poisoning. Its safe use requires concentrated dextrose to prevent fluid overload and strict "permissive hypokalemia" management. GIK is an investigational "metabolic resuscitation" therapy aimed at recruiting hibernating myocardium in septic cardiomyopathy. While potentially beneficial for hypodynamic states, GIK poses a significant risk of severe hypotension in vasoplegic patients due to insulin's vasodilatory effects. Matching the correct insulin strategy to the patient's specific hemodynamic phenotype is critical to maximize efficacy and prevent life-threatening complications.
Downloads
References
Vincent JL, De Backer D. Circulatory shock. N Engl J Med. 2013;369:1726-34.
Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40:1795-815.
Klein LJ, Visser FC. The effect of insulin on the heart: Part 1. Neth Heart J. 2010;18:197-201.
Iliadis F, Kadoglou N, Didangelos T. Insulin and the heart. Diabetes Res Clin Pract. 2011;93:S86-91.
Presneill JJ, Cade JF. Intensive insulin therapy in septic shock. Crit Care Resusc. 2006;8:230-4.
Management of Hyperglycemia in Critical Care. J Diabetes Obes. 2022;13:5.
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
NICE-SUGAR Study Investigators; Finfer S, Chittock DR, Su SY, Blair D, Foster D, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360:1283-97.
Bruns B, Maass C, Barth S, Bruhn A, Duchow J, Vogt A, et al. The role of insulin and glucose handling in takotsubo syndrome. Future Med Inter Cardiol. 2024;21:541.
Bruns B, Joos M, Meder B, Ehlermann P, Frey N, Katus HA, et al. Insulin resistance in Takotsubo syndrome. ESC Heart Fail. 2023;11:796-9.
Shah KR, Przybysz TM, Ushakumari D, Geib AJ. High dose insulin therapy for inotropic support during veno-arterial extracorporeal membrane oxygenation decannulation: A case report. Medicine (Baltimore). 2022;101:e30267.
Yuan TH, Hays HL, Rao RB. High-Dose Insulin Therapy for Calcium Channel Blocker Poisoning: A Review. J Med Toxicol. 2024.
Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47:1181-247.
Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite SS, Deutschman C, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40:3251-76.
Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471-8.
Egi M, Bellomo R, Stachowski E, French CJ, Hart GK, Hegarty C, et al. Blood glucose concentration and outcome of critical illness: the impact of diabetes. Crit Care Med. 2008;36:2249-55.
Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009;32:1119-31.
St-Onge M, Anseeuw K, Cantrell FL, Gilchrist IC, Hantson P, Bailey B, et al. Experts consensus recommendations for the management of calcium channel blocker poisoning in adults. Crit Care Med. 2017;45:e306-15.
Cole JB, Olives TD, Smith SW, Nyström PC, Otto KM. High-dose insulin for beta-blocker and calcium channel blocker poisoning. Am J Emerg Med. 2018;36:1817-24.
DeWitt CR, Waksman JC. Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity. Toxicol Rev. 2004;23:223-38.
Preiser JC, Devos P, Ruiz-Santana S, Melot C, Annane D, Groeneveld J, et al. A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med. 2009;35:1738-48.
Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA. 2008;300:933-44.
Griesdale DE, de Souza RJ, van Dam RM, Heyland DK, Cook DJ, Malhotra A, et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ. 2009;180:821-7.
Kansagara D, Fu R, Freeman M, Wolf F, Helfand M. Intensive insulin therapy in hospitalized patients: a systematic review. Ann Intern Med. 2011;154:268-82.
CREATE-ECLA Trial Group Investigators. Effects of glucose-insulin-potassium infusion on mortality in patients with acute ST-segment elevation myocardial infarction: the CREATE-ECLA randomized controlled trial. JAMA. 2005;293:437-46.
Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94:709-28.
Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med. 2007;35:2262-7.
Egi M, Bellomo R, Stachowski E, French CJ, Hart GK. Hypoglycemia and outcome in critically ill patients. Mayo Clin Proc. 2010;85:217-24.
Kavanagh BP, McCowen KC. Clinical practice. Glycemic control in the ICU. N Engl J Med. 2010;363:2540-6.
Liamis G, Liberopoulos E, Barkas F, Elisaf M. Diabetes mellitus and electrolyte disorders. World J Clin Cases. 2014;2:488-96.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304-77.
Jacobi J. Pathophysiology of sepsis. Am J Health Syst Pharm. 2002;59:S3-8.
Merz TM, Finfer S. Pro/con debate: Is intensive insulin therapy targeting tight blood glucose control of benefit in critically ill patients? Crit Care. 2008;12:211.
Kim JS, Kim YJ, Kim WY. Glucose-insulin-potassium correlates with hemodynamic improvement in patients with septic myocardial dysfunction. J Thorac Dis. 2016;8:3548-56.
Slob E, Shulman R, Singer M. Experience using high-dose glucose-insulin-potassium (GIK) in critically ill patients. J Crit Care. 2017;38:46-8.
Moskowitz A, Andersen LW, Cocchi MN, Karlsson M, ornberg A, Donnino MW. Metabolic resuscitation in sepsis. Chest. 2018;154:1201-11.
Effat H, El-Ghamry R, El-Saeed A. Effect of glucose-insulin-potassium infusion on hemodynamics in patients with septic shock. Open Access Maced J Med Sci. 2021
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

