
Tranexamic acid vs. epsilon-aminocaproic acid: Evidence gaps and practical implications
TXA vs. EACA: Evidence and practice
DOI:
https://doi.org/10.54205/ccc.v34.280593Keywords:
Tranexamic acid, Epsilon-aminocaproic acid, Antifibrinolytic therapy, Perioperative bleeding, Blood conservationAbstract
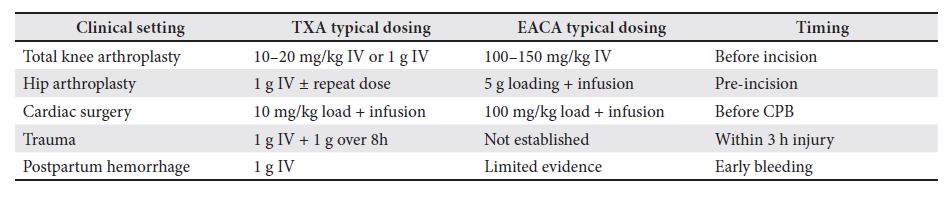
Antifibrinolytic agents, particularly tranexamic acid (TXA) and epsilon-aminocaproic acid (EACA), are widely used to reduce perioperative bleeding. Although both drugs share a similar mechanism—competitive inhibition of plasminogen activation—they differ in pharmacologic potency, dosing requirements, and clinical evidence. TXA demonstrates 6–10 times greater affinity for plasminogen, resulting in stronger antifibrinolytic effects at lower doses. Evidence from randomized trials and meta-analyses, primarily in orthopedic surgery, suggests TXA may reduce blood loss more effectively than EACA; however, differences in transfusion rates and thromboembolic complications are generally not significant. In cardiac surgery, limited data show no clear superiority of either agent. TXA has robust evidence supporting its use in trauma and obstetrics, while comparable high-quality data for EACA remain lacking. Both agents appear safe, though high doses—especially in renal impairment—may increase seizure risk. Importantly, EACA may achieve similar clinical outcomes when administered at appropriately higher doses. Current evidence is limited by heterogeneous study designs, variable dosing regimens, and underpowered trials. Overall, while TXA is more potent and better studied, definitive clinical superiority over EACA remains unproven. Drug selection should therefore consider patient factors, institutional protocols, and resource availability pending further large-scale comparative trials.
Downloads
References
Zheng C, Ma J, Xu J, Li M, Wu L, Wu Y, et al. The optimal dose, efficacy and safety of tranexamic acid and epsilon-aminocaproic acid to reduce bleeding in TKA: A systematic review and bayesian network meta-analysis. Orthop Surg. 2023;15:930–46.
Patel PA, Wyrobek JA, Butwick AJ, Pivalizza EG, Hare GMT, Mazer CD, et al. Update on applications and limitations of perioperative tranexamic acid. Anesth Analg. 2022;135:460–73.
Yusufu A, Haibier A, Ren Z, Qin Q, Zhang Z, Zhou Y, et al. Efficacy and safety of using aminocaproic acid and tranexamic acid during the perioperative period for treating trochanteric fractures in elderly femurs. BMC Musculoskelet Disord. 2023;24:546.
Bradley KE, Ryan SP, Penrose CT, Grant SA, Wellman SS, Attarian DE, et al. Tranexamic acid or epsilon-aminocaproic acid in total joint arthroplasty? A randomized controlled trial. Bone Joint J. 2019;101-B:1093–9.
Boese CK, Centeno L, Walters RW. Blood conservation using tranexamic acid is not superior to epsilon-aminocaproic acid after total knee arthroplasty. Journal of Bone and Joint Surgery. 2017;99:1621–8.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

