
Comparison of Procaine and Lidocaine in Cardioplegia for Preventing Ventricular Fibrillation After Aortic Cross-Clamping Release in Coronary Artery Bypass Graft
Keywords:
Coronary artery bypass graft, Lidocaine hydrochloride, Procaine hydrochloride, Ventricular fibrillationAbstract
Background: The use of procaine hydrochloride in cardioplegia has been discontinued due to challenges importing the product from outside the country despite its crucial role in preserving myocardium during heart surgery. However, lidocaine hydrochloride, an anti-arrhythmic medication, functions similarly to procaine hydrochloride. Both medications are compared regarding their effectiveness in preventing ventricular fibrillation, the most common type of heart arrhythmia, after releasing the aortic cross-clamp in cardiac surgery.
Materials and Methods: This is a retrospective study in which data were collected from medical records of patients who were operated on with coronary artery bypass grafts between May 2017 and August 2023. Patient demographics and early outcomes between the two groups were analyzed.
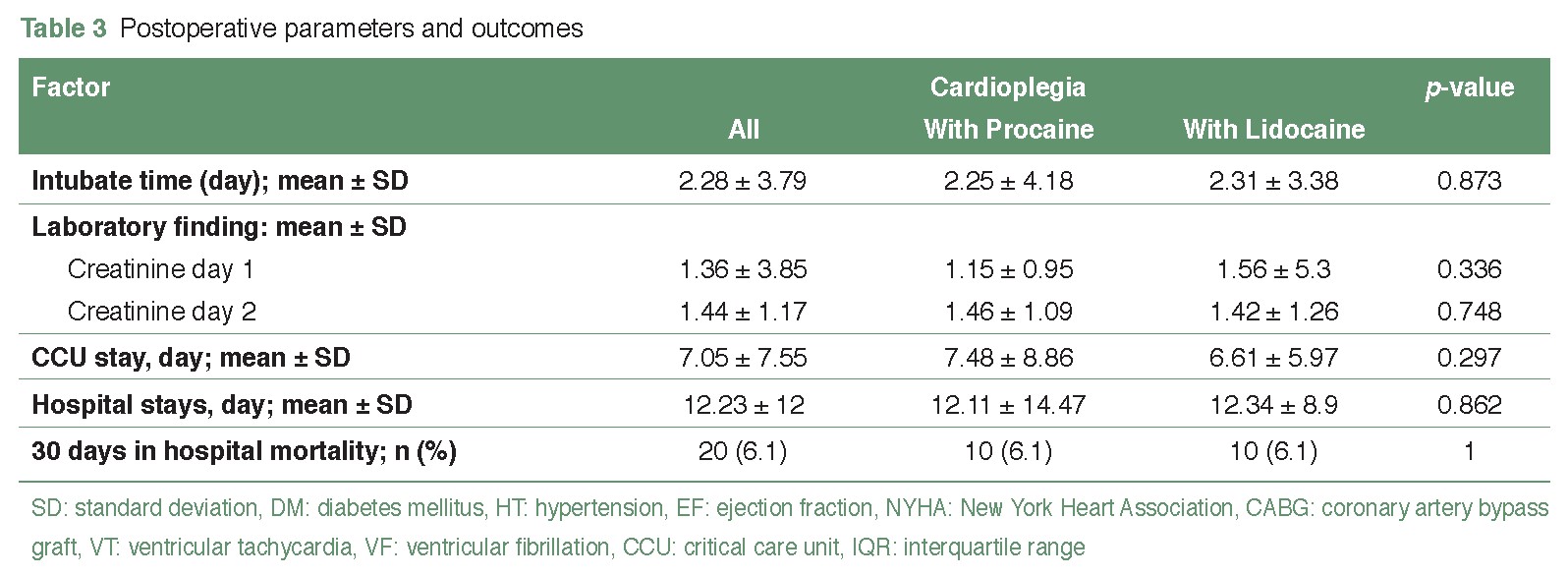
Results: A total of 328 patients who operated on CABG were divided into 2 groups, respectively. Group one was a group of cardioplegia solutions with procaine hydrochloride, and group two was a group of cardioplegia solutions with lidocaine hydrochloride. Most participants were 64.19 years old and 64.24 years old, respectively. The duration of the aortic cross-clamp was significantly different between the two groups, with durations of 76.06 minutes and 87.79 minutes, respectively, showing a p-value of less than 0.01 in statistical analysis. Following the release of aortic cross-clamping, the occurrence of ventricular fibrillation was observed in 37 patients (43%) in the first group and 49 patients (56.9%) in the second group, with no significant difference noted. Subsequent to defibrillation at 10 joules, there were 21 patients (24.4%) in the first group and 13 patients (15.1%) in the second group, indicating a significant difference. Additionally, no significant difference was observed in the duration of the CCU stay between both groups.
Conclusion: Cardioplegic solution containing lidocaine hydrochloride provides the same clinical result as procaine hydrochloride in coronary artery bypass grafting surgery.
References
Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke statistics—2015 Update. A report from the American Heart Association. Circulation. 2015;131(4):434-41. doi: 10.1161/CIR.0000000000000157.
Chung M, Asher R, Yamada D, et al. Arrhythmias after cardiac and non-cardiac surgery. In: Podrid P, Kowey P, editors. Cardiac arrhythmia. 2nd ed. Philadelphia: Lippincott Williams Wilkins. 2001:631-8.
Braunwald E, Zipes DP, Libby P. Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia: Saunders. 2001:833-55.
Ibrahim MF, Venn GE, Young CP, et al. A clinical comparative study between crystalloid and blood-based St Thomas' hospital cardioplegic solution. Eur J Cardiothorac Surg. 1999;15(1):75-83. doi: 10.1016/s1010-7940(98)00287-5.
Matte GS, del Nido PJ. History and use of del Nido cardioplegia solution at Boston Children's Hospital. J Extra Corpor Technol. 2012;44(3):98-103.
Sellevold OF, Berg EM, Levang OW. Procaine hydrochloride in cardioplegia (CPL): An effective drug in reducing postischaemic ventricular fibrillation in man. J Cardiothorac Vasc Anesth. 1994;8(3):69. doi:10.1016/1053-0770(94)90472-3.
Goldstone AB, Bronster DJ, Anyanwu AC, et al. Predictors and outcomes of seizures after cardiac surgery: a multivariable analysis of 2,578 patients. Ann Thorac Surg. 2011;91(2):514-8. doi: 10.1016/j.athoracsur.2010.10.090.
Alex J, Bhamra GS, Cale AR, et al. Atrial fibrillation after coronary bypass surgery- pathophysiology, resource utilization and management strategies. Br J Cardiol. 2003;10:82–8.
Wu ZK, Iivainen T, Pehkonen E, et al. Fibrillation in patients subjected to coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;126(5):1477-82. doi: 10.1016/s0022-5223(03)00749-9.
Banach M, Rysz J, Drozdz JA, et al. Risk factors of atrial fibrillation following coronary artery bypass grafting: a preliminary report. Circ J. 2006;70(4):438-41. doi: 10.1253/circj.70.438.
Doherty PW, McLaughlin PR, Billingham M, et al. Cardiac damage produced by direct current countershock applied to the heart. Am J Cardiol. 1979;43(2):225-32. doi: 10.1016/s0002-9149(79)80008-9.
Komori S, Sano S, Li BH, et al. Effects of bidisomide (SC-40230), a new class I antiarrhythmic agent, on ventricular arrhythmias induced by coronary artery occlusion and reperfusion in anesthetized rats; comparison with mexiletine and disopyramide. Heart Vessels. 1995;10(1):7-11. doi: 10.1007/BF01745072.
Elnakera AM, Alawady TSM. Continuous infusion of magnesium–lidocaine mixture for prevention of ventricular arrhythmias during on-pump coronary artery bypass grafting surgery. Egypt J Anaesth. 2013;29(4):419–25. doi: 10.1016/j.egja.2013.05.002.
Peretto G, Durante A, Limite LR, et al. Postoperative arrhythmias after cardiac surgery: incidence, risk factors, and therapeutic management. Cardiol Res Pract. 2014;2014:615987. doi: 10.1155/2014/615987.
Dorian P, Fain ES, Davy JM, et al. Lidocaine causes a reversible, concentration-dependent increase in defibrillation energy requirements. J Am Coll Cardiol. 1986;8(2):327-32. doi: 10.1016/s0735-1097(86)80047-x.
Balachandran V, Zhou X, Huang L, et al. A comparison of the effects of lidocaine or procaine containing St. Thomas no. 2 cardioplegia solution on post-operative renal function. Cardiol Cardiovasc Med. 2020;4(2):105-10.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 The Royal College of Surgeons of Thailand

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles must be contributed solely to The Thai Journal of Surgery and when published become the property of the Royal College of Surgeons of Thailand. The Royal College of Surgeons of Thailand reserves copyright on all published materials and such materials may not be reproduced in any form without the written permission.

