
Prone positioning reduces ARDS mortality: A meta-analysis for ICU teams
Prone positioning meta-analysis for ARDS
DOI:
https://doi.org/10.54205/ccc.v34.281631Keywords:
Acute respiratory distress syndrome, Prone positioning, Mortality, Meta-analysis, Multidisciplinary team, Resource-limited settingsAbstract
Background: Prone positioning has been utilized as adjunctive therapy for acute respiratory distress syndrome (ARDS) for decades. However, the magnitude of mortality reduction has remained uncertain, particularly after publication of multiple randomized controlled trials during the COVID-19 pandemic.
Method: We performed a systematic review and meta-analysis following PRISMA 2020 guidelines and registered in PROSPERO (CRD420261360074) with analyses prespecified. We searched PubMed, Cochrane CENTRAL, CINAHL, Google Scholar, and ThaiJO from January 1, 2016 through March 31, 2026, supplemented by hand-searching of references (including four pre-2016 trials). We included randomized controlled trials comparing prone positioning to supine positioning in adults with ARDS (Berlin or 2024 criteria). Primary outcome was 28-day or hospital mortality acknowledged as a limitation. We used a random-effects model to calculate risk ratios (RR) with 95% confidence intervals (CI). Risk of bias was assessed with ROB-2; certainty of evidence with GRADE.
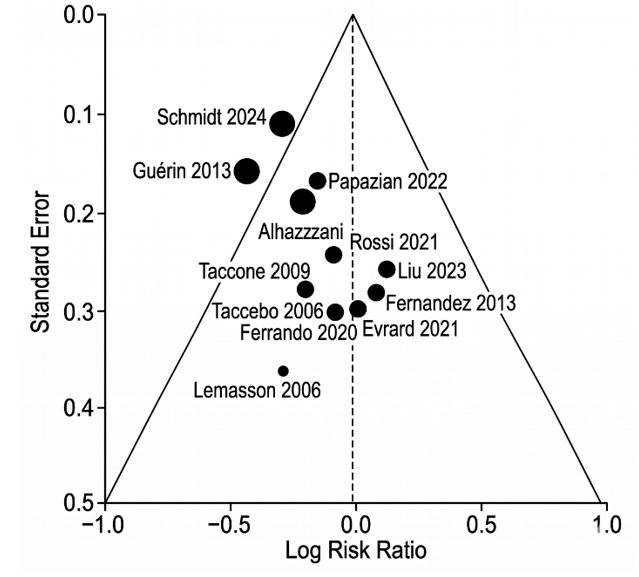
Result: Twelve randomized controlled trials (3,247 patients) met eligibility criteria. Prone positioning significantly reduced mortality compared to supine positioning (RR 0.74, 95% CI 0.65 to 0.84, p<0.001; I²=48%). Benefit was greater in severe ARDS (PaO₂/FiO₂ ≤100 mm Hg; RR 0.66, 95% CI 0.55 to 0.79; number needed to treat [NNT]=6). Prone duration ≥16 hours/day was associated with greater mortality reduction (RR 0.68, 95% CI 0.58 to 0.80) compared to shorter durations (RR 0.88, 95% CI 0.73 to 1.06; interaction p=0.03). Benefit was consistent between COVID-19 and non-COVID-19 etiologies (p=0.58). Prone positioning increased pressure injury incidence (RR 2.34, 95% CI 1.78 to 3.08; number needed to harm=7). Severe pressure injuries (stage 3 or 4) were rare (0.9% of prone patients). Certainty of evidence was moderate for mortality and high for pressure injuries.
Conclusion: Prone positioning reduces mortality in adult ARDS, particularly severe disease and when implemented for ≥16 hours/day. Successful implementation requires coordinated multidisciplinary team action.
Registration:This study is part of a project registered with PROSPERO (CRD420261360074) as 'Development of Clinical Nursing Practice Guidelines for Patients with Acute Respiratory Distress Syndrome (ARDS): A Synthesis of Empirical Evidence for Clinical Practice in the Thai Context'.
Downloads
References
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788-800.
Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-68.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-33.
Matthay MA, Arabi YM, Siegel ER, Ware LB, Bos LDJ, Sinha P, et al. A new global definition of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2024;209(1):37-47.
Taccone P, Pesenti A, Latini R, Polli F, Vagginelli F, Mietto C, et al. Prone positioning in patients with moderate and severe acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2009;302(18):1977-84.
Mancebo J, Fernández R, Blanch L, Rialp G, Gordo F, Ferrer M, et al. A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 2006;173(11):1233-9.
Lemasson S, Ayzac L, Girard R, Gaillard P, Pavaday K, Guérin C. Does prone positioning increase the risk of pressure ulcers in patients with acute respiratory distress syndrome? Intensive Care Med. 2006;32(6):868-73.
Munshi L, Del Sorbo L, Adhikari NKJ, Hodgson CL, Wunsch H, Meade MO, et al. Prone position for acute respiratory distress syndrome: a systematic review and meta-analysis. Ann Am Thorac Soc. 2017;14(Suppl 4):S280-8.
Sud S, Friedrich JO, Adhikari NKJ, Taccone P, Mancebo J, Polli F, et al. Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis. CMAJ. 2014;186(10):E381-90.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Thai Society of Critical Care Medicine

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.

