Factors Associated with False Positive Treadmill Exercise Stress Test Results
Keywords:
exercise stress test, coronary computed tomography angiography, coronary angiographyAbstract
Background: The treadmill exercise stress test (EST) is predominantly performed in patients who are symptomatic or suspected of having ischemic heart disease. This study was conducted to study the factors associated with false positive EST results for CAD.
Methods: This was a cross-sectional study. Patients who obtained a positive EST result at the Cardiovascular Division, Department of Internal Medicine, Phramongkutklao Hospital, and who subsequently underwent coronary angiography (CAG) or coronary computed tomography angiography (CCTA) between October 2013 and October 2016 were included. Patients were divided into two groups, true positive and false positive, depending upon the CCTA and CAG data. The two groups were compared with each other.
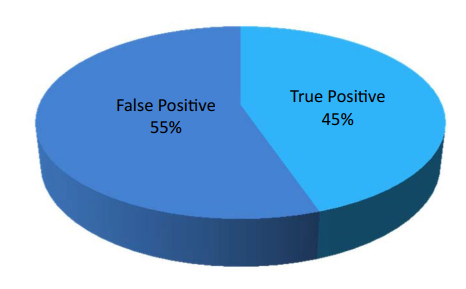
Results: One hundred and seventy-two patients were included, 67% of whom were male. Ninety-five (55.2%) patients, most of whom were male (65.3%), had a false positive EST result. The mean age in the true positive group was 64.6 years, and that in the false positive group was 59.7 years. There was no significant difference in blood pressure response between the two groups. In the univariate analysis, in female patients, risk factors, including diabetes and dyslipidemia, appropriate heart rate responsiveness, upslope ST depression, and downslope ST segment depression confined to the inferior leads, had a statistically significant correlation between groups. Multivariate analysis to determine the independent predictors of a false positive EST result identified female sex (odds ratio [OR], 3.90; 95% confidence interval [CI], 1.36–11.18; p = 0.011) and upslope ST segment depression (OR, 74.03; 95% CI, 7.74–707.65; p < 0.001). The most commonly involved vessel was the left anterior descending artery (62, 81.58%), followed by the right coronary artery (52, 67.53%), and the left circumflex artery (49, 63.64%).
Conclusions: Female sex and upslope ST segment depression are associated with false positive EST results.
Downloads
References
Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct?. Chest. 2000;118(2):535-541.doi:10.1378/chest.118.2.535 https://doi.org/10.1378/chest.118.2.535 PMid:10936152
Zipes DP, Libby P, Bonow RO, Braunwald E. Exercise stress testing, In Braunwald's Heart Disease.10th ed 2015; Philadelphia Elsevier Saunders: p155-178.
Kern MJ, Samady H. Current concepts of integrated coronary physiology in the catheterization laboratory. J Am Coll Cardiol. 2010;55(3):173-185. doi:10.1016/j.jacc.2009.06.062 https://doi.org/10.1016/j.jacc.2009.06.062 PMid:20117397
Kwok YS, Kim C, Grady D, Redberg RF. Exercise testing for coronary artery disease diagnosis in women: a meta analysis. Circulation. 1995;94:I-497.
Zhao D, Freeman DH, de Flippi CR. A metaanalysis of gender differences in exercise testing. Circulation. 1995;94:I-497.
Walling AD, Crawford MH. Exercise testing in women with chest pain: applications and limitations of computer analysis. Coron Artery Dis. 1993;4(9):783-789. doi: 10.1097/00019501-199309000-00005 https://doi.org/10.1097/00019501-199309000-00005 PMid:8287212
Okin PM, Kligfield P. Identifying coronary artery disease in women by heart rate adjustment of ST-segment depression and improved performance of linear regression over simple averaging method with comparison to standard criteria. Am J Cardiol.1992; 69(4):297-302.doi:10.1016/0002-9149(92) 90223-l https://doi.org/10.1016/0002-9149(92)90223-L
Robert AR, Melin JA, Detry JM. Logistic discriminant analysis improves diagnostic accuracy of exercise testing for coronary artery disease in women. Circulation. 1991; 83(4):1202-1209.doi:10.1161/01.CIR.83.4.1202 https://doi.org/10.1161/01.CIR.83.4.1202 PMid:2013142
Hachamovitch R, Berman DS, Kiat H, et al. Effective risk stratification using exercise myocardial perfusion SPECT in women: gender-related differences in prognostic nuclear testing. J Am Coll Cardiol. 1996;28(1):34-44. doi:10.1016/0735-1097(96)00095-2 https://doi.org/10.1016/0735-1097(96)00095-2
Morise AP, Diamond GA, Detrano R, Bobbio M.Incremental value of exercise electrocardiography and thallium-201 testing in men and women for the presence and extent of coronary artery disease. Am Heart J. 1995;130(2):267-276. doi:10.1016/0002- 8703(95)90439-5 https://doi.org/10.1016/0002-8703(95)90439-5
Williams MJ, Marwick TH, O'Gorman D, Foale RA. Comparison of exercise echocardiography with an exercise score to diagnose coronary artery disease in women. Am J Cardiol. 1994;74(5):435-438. doi:10.1016/ 0002-9149(94)90898-2 https://doi.org/10.1016/0002-9149(94)90898-2
Bickell NA, Pieper KS, Lee KL, et al. Referral patterns for coronary artery disease treatment: gender bias or good clinical judgment?. Ann Intern Med. 1992;116(10):791- 797. doi:10.7326/0003-4819-116-10-791 https://doi.org/10.7326/0003-4819-116-10-791 PMid:1567093
Alexander KP, Shaw LJ, Shaw LK, Delong ER, Mark DB, Peterson ED. Value of exercise treadmill testing in women [published correction appears in J Am Coll Cardiol 1999 Jan;33(1):289]. J Am Coll Cardiol.1998;32(6):1657-1664. doi:10.1016/s0735-1097(98)00451-3 https://doi.org/10.1016/S0735-1097(98)00451-3
Gibbons RJ, Balady GJ, Beasley JW, et al. ACC/AHA guidelines for exercise testing: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). Circulation. 1997;96(1):345-354.doi:10.1161/01.cir.96.1.345 https://doi.org/10.1161/01.CIR.96.1.345 PMid:9236456
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Chulabhorn Royal Academy

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright and Disclaimer
Articles published in this journal are the copyright of Chulabhorn Royal Academy.
The opinions expressed in each article are those of the individual authors and do not necessarily reflect the views of Chulabhorn Royal Academy or any other faculty members of the Academy. The authors are fully responsible for all content in their respective articles. In the event of any errors or inaccuracies, the responsibility lies solely with the individual authors.

