
Effects of Pharmaceutical Care on Clinical Outcomes in Patients with Chronic Kidney Disease in Wiang Haeng Hospital, Chiang Mai Province
Keywords:
Chronic Kidney Disease, Pharmaceutical Care, Clinical OutcomesAbstract
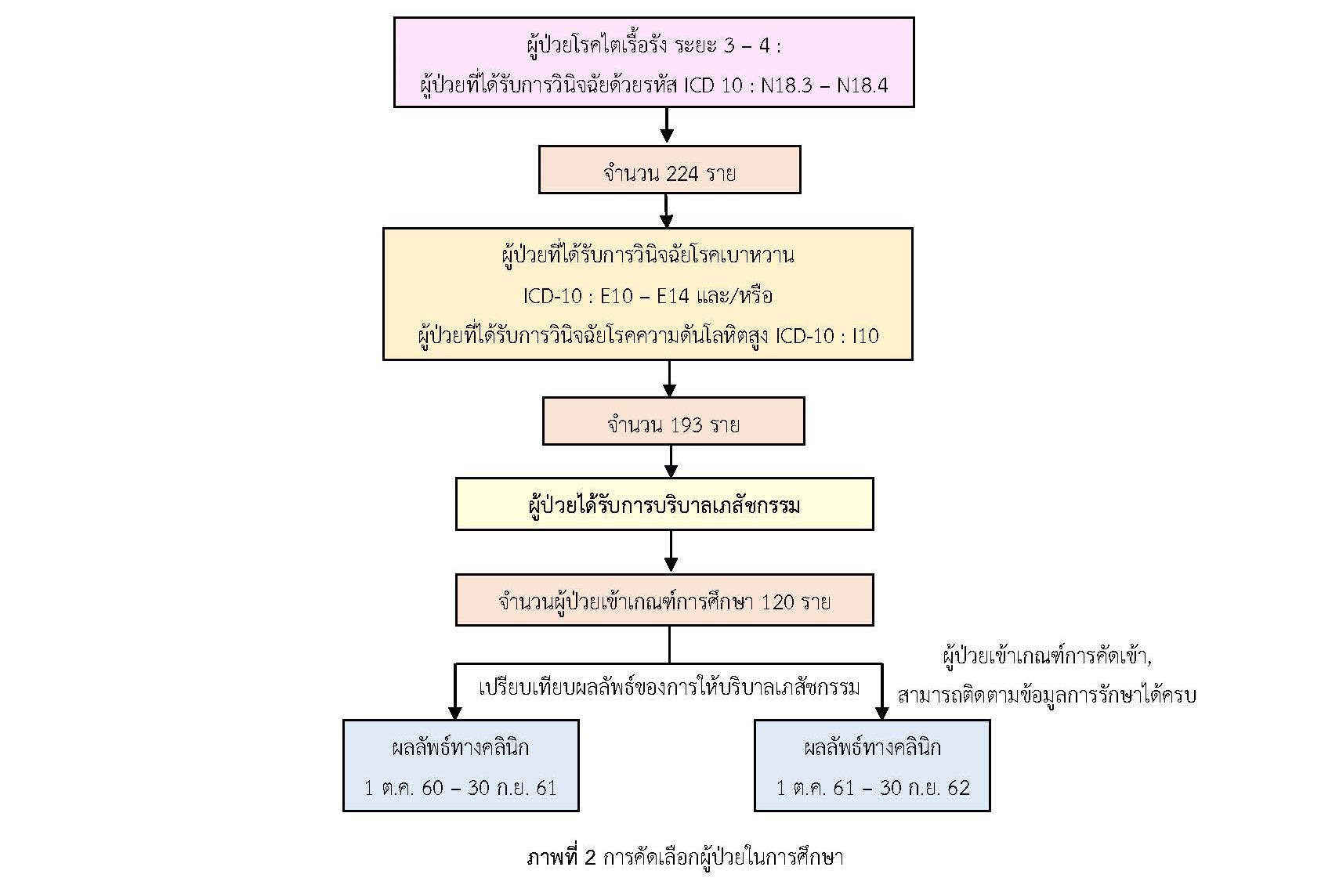
The objective of this retrospective study was to examine the effects of a pharmaceutical care program on clinical outcomes in patients with stage 3 or 4 Chronic Kidney Disease (CKD) and having diabetes mellitus or hypertension or both as co-morbidities. The pharmaceutical care program included finding drug-related problems, assessing medical adherence, reviewing prescription, adjusting a drug's dosage, and guiding on drug education. The study was conducted by studying medical records between October 1, 2017 and September 30, 2019. The study was to compare clinical outcomes in a single group of participants before and after receiving a pharmaceutical care program for a one-year period that started from October 1, 2018. Clinical outcomes, included levels of blood pressure, blood pressure (BP), fasting blood sugar (FBS), glycosylated hemoglobin (HbA1C), total cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL) and low-density lipoprotein (LDL). Data was analyzed by descriptive analysis. Paired t-test was used to compare kidney function blood values before and after receiving a pharmaceutical care program.
The study showed that the average age of patients was 71 years old (S.D.=10.7) and 51.7% were females. Most of patients (95.8%) were at stage 3 CKD. The average estimated glomerular filtration rate (eGFR) was significantly improved around 51.85 (S.D.=14.71) at baseline testing to 54.84 (S.D.=16.53) ml/min/1.73m2 at 12-month follow up (p-value=0.009). The average serum creatinine level had decreased significantly from 1.33 (S.D.=0.41) at the baseline to 1.27 (S.D.=0.39) mg/dL at 12-month follow up (p-value=0.001). This study suggested that the pharmaceutical care program is an effective tool to slow the deterioration rate of kidney function in patients with CKD and having diabetes mellitus or hypertension or both as co-morbidities.
References
กระทรวงสาธารณสุข. (2565). KPI กระทรวงสาธารณสุข: ร้อยละผู้ป่วย CKD ที่มีค่า eGFR ลดลงน้อยกว่าหรือเท่ากับ 5 ml/min/1.73 m2/yr. สืบค้นเมื่อ 22 ตุลาคม 2565 จากhttp://healthkpi.moph.go.th/kpi2/kpi-list/view/?id=1857.
กานต์ธีรา ชัยเรียบ ภัทรินทร์ กิตติบุญญาคุณ และวนรัตน์ อนุสรณ์เสงี่ยม. (2560). การพัฒนารูปแบบการบริบาลทางเภสัชกรรมร่วมกับทีมสหสาขาวิชาชีพในการดูแลผู้ป่วยไตวายระยะสุดท้ายที่ได้รับการรักษาโดยการฟอกเลือดด้วยเครื่องไตเทียมทั้งในโรงพยาบาลและการดูแลที่บ้าน. วารสารเภสัชกรรมไทย, 10(2), 324-336.
จักรภพ สวัสดิ์พาณิชย์. (2557). การบริบาลทางเภสัชกรรมเบื้องต้นในผู้ป่วยโรคไตเรื้อรัง โรงพยาบาลกันทรวิชัย จังหวัดมหาสารคาม. วารสารวิจัยและพัฒนาระบบสุขภาพ, 7(3), 57-63.
นีลนาถ เจ๊ะยอ และอนุชิต วังทอง. (2552). ผลของการใช้ยาเบาหวานตามแนวทางปฏิบัติของ NKF-K/DOQI ในผู้ป่วยโรคเบาหวานที่มีภาวะไตวายเรื้อรังระยะที่ 3-5. สงขลานครินทร์เวชสาร, 27(4), 271-278.
ประเสริฐ ธนะกิจจารุ, สกานต์ บุนนาค และวรางคณา พิชัยวงศ์. (2557). โรคไตเรื้อรัง (Chronic Kidney Disease). ใน ชุษณะ มะกรสาร (บ.ก.), Thailand Medical Services Profile 2011 – 2014 (การแพทย์ไทย 2554-2557). นนทบุรี: กรมการแพทย์ กระทรวงสาธารณสุข.
พนาวัลย์ ศรีสุวรรณภพ. (2555). ประสิทธิผลของการดูแลผู้ป่วยโรคไตเรื้อรังในคลินิกเบาหวาน โรงพยาบาลชาติตระการ. วิทยานิพนธ์ปริญญาเภสัชศาสตรมหาบัณฑิต. มหาวิทยาลัยศิลปากร.
พัชนี นวลช่วย. (2555). ผลของการให้บริบาลทางเภสัชกรรมต่อการควบคุมปัจจัยเสี่ยงต่อการเสื่อมของไต ในผู้ป่วยโรคไตเรื้อรัง ณ โรงพยาบาลท่าศาลา. วิทยานิพนธ์ปริญญาเภสัชศาสตรมหาบัณฑิต. มหาวิทยาลัยสงขลานครินทร์.
วรรณคล เชื้อมงคล, ปิยวดี สุขอยู่ และนลินี เครือทิวา. (2557). ผลการให้คำปรึกษาด้านยาแก่ผู้ป่วยโรคไตเรื้อรังระยะสุดท้าย ที่ได้รับการบำบัดทดแทนไตด้วยการล้างไตทางช่องท้องต่อความร่วมมือในการใช้ยาที่คลินิกบำบัดทดแทนไต โรงพยาบาลนพรัตนราชธานี กรุงเทพมหานคร. วารสารเภสัชศาสตร์อีสาน, 10(3), 339-353.
สมาคมโรคไตแห่งประเทศไทย. (2558). คำแนะนำสำหรับการดูแลผู้ป่วยโรคไตเรื้อรังก่อนการบำบัดทดแทนไต พ.ศ.2558.
สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข. (2561). สรุปรายงาน การเฝ้าระวังโรคประจำปี 2560 (Annual Epidemiological Surveillance Report 2018). กรุงเทพฯ: กองระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข.
สุธาบดี ม่วงมี. (2559). ผลของการบริบาลทางเภสัชกรรมต่อการชะลอไตเสื่อมของไตในผู้ป่วยโรคไตเรื้อรังร่วมกับโรคเบาหวานชนิดที่ 2. วิทยานิพนธ์ปริญญาเภสัชศาสตรมหาบัณฑิต. มหาวิทยาลัยศิลปากร.
อุไรวรรณ พานทอง. (2561). การจัดการโรคไตเรื้อรังโดยใชรูปแบบการดูแลโรคเรื้อรังในสถานบริการปฐมภูมิจังหวัดนครศรีธรรมราช. มหาราชนครศรีธรรมราชเวชสาร, 1(2), 48-58.
Al Raiisi, F., Stewart, D., Fernandez-Llimos, F., Salgado, T. M., Mohamed, M. F., & Cunningham, S. (2019). Clinical pharmacy practice in the care of Chronic Kidney Disease patients: a systematic review. International Journal of Clinical Pharmacy, 41(3), 630–666.
Alruqayb, W. S., Price, M. J., Paudyal, V., & Cox, A. R. (2021). Drug-Related Problems in Hospitalised Patients with Chronic Kidney Disease: A Systematic Review. Drug Safety, 44(10), 1041–1058.
Ameh, O. I., Ekrikpo, U. E., & Kengne, A. P. (2019). Preventing CKD in Low- and Middle-Income Countries: A Call for Urgent Action. Kidney International Reports, 5(3), 255–262.
Anderegg, M. D., et al. (2018). Pharmacist Intervention for Blood Pressure Control in Patients with Diabetes and/or Chronic Kidney Disease. Pharmacotherapy, 38(3), 309–318.
Casas, J. P., et al. (2005). Effect of inhibitors of the renin-angiotensin system and other antihypertensive drugs on renal outcomes: Systematic review and meta-analysis. Lancet (London, England), 366, 2026-2033.
Cha'on, U., et al. (2020). CKDNET, a quality improvement project for prevention and reduction of chronic kidney disease in the Northeast Thailand. BMC Public Health, 20(1), 1299.
Ingsathit, A., et al. (2010). Prevalence and risk factors of chronic kidney disease in the Thai adult population: Thai SEEK study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association, 25(5), 1567–1575.
Jha, V., et al. (2013). Chronic kidney disease: global dimension and perspectives. Lancet (London, England), 382(9888), 260-272.
Kalantar-Zadeh, K., Jafar, T. H., Nitsch, D., Neuen, B. L., & Perkovic, V. (2021). Chronic kidney disease. Lancet (London, England), 398(10302), 786–802.
Kasbekar, R., & Ambizas, E. M. (2021). Chronic Kidney Disease. US Pharmacist, 45(3), 6-12.
Kovesdy, C. P. (2022). Epidemiology of chronic kidney disease: An update 2022. Kidney International Supplements, 12(1), 7–11.
Kshirsagar, A. V., Joy, M. S., Hogan, S. L., Falk, R. J., & Colindres, R., E. (2000). Effect of ACE inhibitors in diabetic and nondiabetic chronic renal disease: a systematic overview of randomized placebo-controlled trials. American Journal of Kidney Diseases: The Official Journal of The National Kidney Foundation, 35(4), 695-707.
Paini, A., Salvetti, M., Caligaris, S., Castelli, F., & Muiesan, M. L. (2019). Chronic kidney disease in low-middle income populations: A call to action for screening and prevention. Internal and Emergency Medicine, 14(2), 199–202.
Strippoli, G. F., Bonifati, C., Craig, M., Navaneethan, S. D., & Craig, J. C. (2006). Angiotensin converting enzyme inhibitors and angiotensin II receptor antagonists for preventing the progression of diabetic kidney disease (Review). The Cochrane Database of Systematic Reviews, 2006(4), CD006257.
Webster, A. C., Nagler, E. V., Morton, R. L., & Masson, P. (2017). Chronic kidney disease. Lancet (London, England), 389(10075), 1238–1252.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Journal of Nursing and Public Health Research

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
1. บทความหรือข้อคิดเห็นใด ๆ ที่ปรากฏในวารสารวิจัยการพยาบาลและการสาธารณสุข ที่เป็นวรรณกรรมของผู้เขียน บรรณาธิการไม่จำเป็นต้องเห็นด้วย
2. บทความที่ได้รับการตีพิมพ์ถือเป็นลิขสิทธิ์ของ วารสารวิจัยการพยาบาลและการสาธารณสุข




