
ผลของการฝึกหายใจแบบช้าต่อการขยายตัวของทรวงอก สมรรถภาพปอด และการฟื้นตัวของอัตราการเต้นของหัวใจในผู้ที่เป็นโรคอ้วน อายุ 18-35 ปี
คำสำคัญ:
โรคอ้วน, ปริมาตรของอากาศที่เป่าออกอย่างเร็วแรง, อัตราการเต้นของหัวใจภายหลังออกกำลังกาย, การหายใจแบบช้าบทคัดย่อ
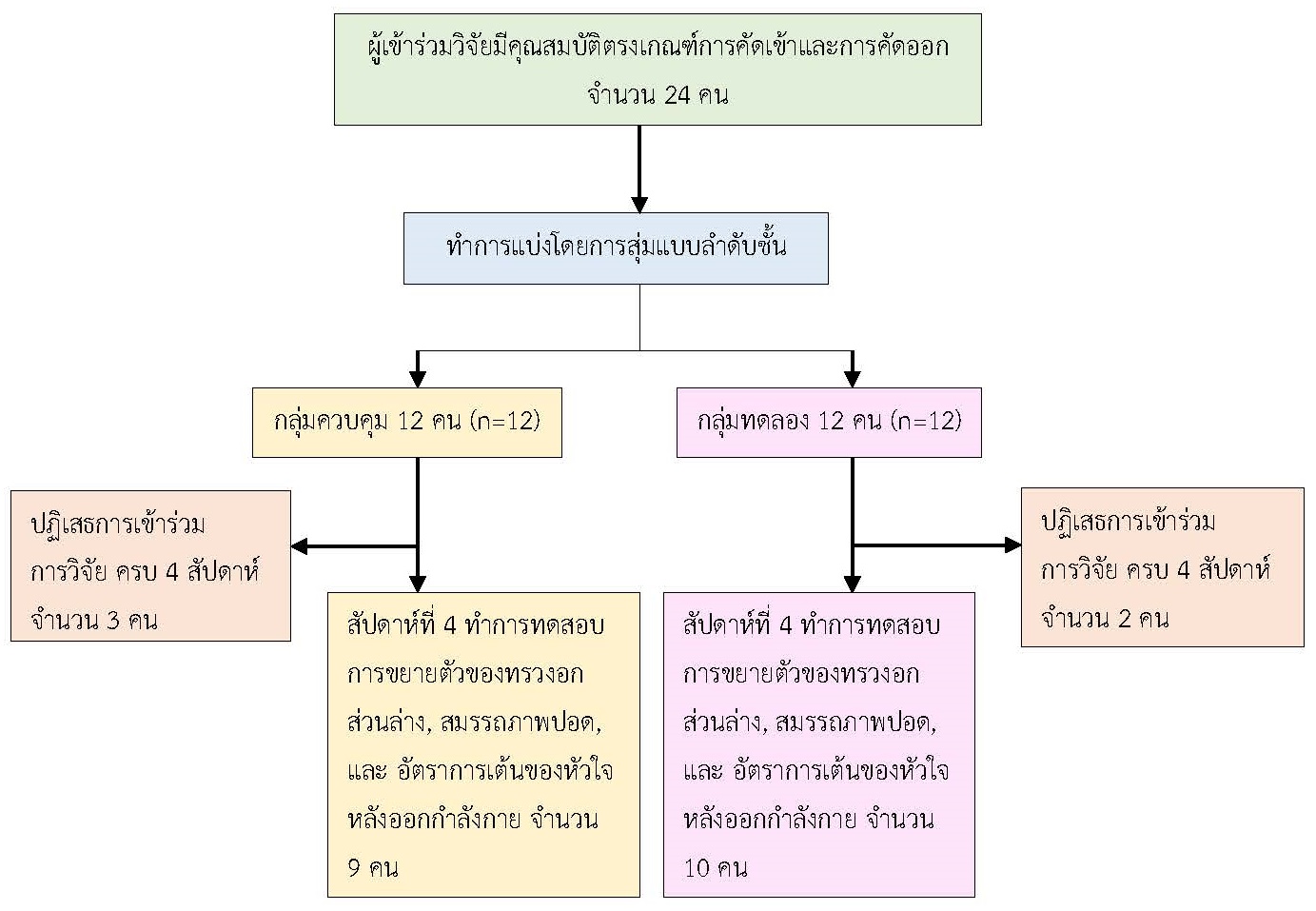
การวิจัยเชิงทดลองนี้มีวัตถุประสงค์เพื่อศึกษาการเปลี่ยนแปลงการขยายตัวของทรวงอก สมรรถภาพปอด และการฟื้นตัวของอัตราการเต้นของหัวใจในผู้ที่เป็นโรคอ้วน ภายหลังการฝึกหายใจแบบช้าโดยใช้กล้ามเนื้อกระบังลมเป็นระยะเวลา 4 สัปดาห์ ผู้เข้าร่วมวิจัยเป็นกลุ่มบุคคลที่เป็นโรคอ้วน มีช่วงอายุระหว่าง 18-35 ปี จำนวน 19 คน แบ่งเป็น 2 กลุ่ม ด้วยวิธีการสุ่มแบบลำดับชั้น ได้แก่ กลุ่มควบคุม จำนวน 9 คน โดยดำรงพฤติกรรมสุขภาพเดิม เป็นระยะเวลา 4 สัปดาห์ และกลุ่มทดลอง จำนวน 10 คน ทำฝึกการหายใจแบบช้าโดยใช้กล้ามเนื้อกะบังลม (Diaphragmatic Breathing Exercise (DBE)) จำนวน 6 ครั้ง ใน 1 นาที พัก 1 นาที ฝึก 10 นาที/ครั้ง ทำทุกวัน เป็นระยะเวลา 4 สัปดาห์ ทั้ง 2 กลุ่มได้รับประเมินการขยายของทรวงอก (Chest Expansion) ร้อยละของปริมาตรอากาศจากการเป่าออกอย่างแรงและเร็วจนหมดหลังการหายใจเข้าเต็มที่ (%Predicted Forced Vital Capacity (FVC)) ร้อยละของปริมาตรของอากาศที่เป่าออกอย่างเร็วแรงในวินาทีที่ 1 (%Predicted Forced Expiratory Volume in One Second (FEV1)) ร้อยละของปริมาตรของอากาศที่เป่าออกมาได้ในวินาทีที่ 1 ต่อปริมาตรของอากาศที่เป่าออกมาได้มากที่สุดอย่างเร็วแรง (%Predicted of the Ratio of the Forced Expiratory Volume in One Second to the Forced Vital Capacity (%FEV1/FVC)) ปริมาตรอากาศทั้งหมดที่หายใจเข้าออกเต็มที่ในเวลา 1 นาที (Predicted Maximal Voluntary Ventilation (MVV)) และการฟื้นตัวของอัตราการเต้นของหัวใจ (Heart Rate Recovery (HRR)) ก่อนและหลังการทดลองเป็นระยะเวลา 4 สัปดาห์ วิเคราะห์ข้อมูลโดยใช้สถิติการวิเคราะห์ความแปรปรวนสองทาง (Two-way ANOVA)
ผลการวิจัย พบว่า เมื่อเปรียบเทียบผลก่อนและหลังการทดลองเป็นระยะเวลา 4 สัปดาห์ กลุ่มทดลองมีค่าเฉลี่ยการขยายตัวของทรวงอกส่วนล่างเพิ่มขึ้นอย่างมีนัยสำคัญทางสถิติ (ก่อนการทดลอง: Mean ± SEM=2.20 ± 0.32 cm, หลังการทดลอง: Mean ± SEM= 2.95 ± 0.24 cm, p-value = 0.001) และกลุ่มควบคุม มีค่า %Predicted FVC ลดลงอย่างมีนัยสำคัญทางสถิติ (ก่อนการทดลอง: Mean ± SEM=101± 3.45, หลังการทดลอง: Mean ± SEM= 96.70 ± 3.32, p-value = 0.001) แต่ไม่พบความแตกต่างกันอย่างมีนัยสำคัญทางสถิติของการเปลี่ยนแปลงค่า %Predicted FEV1/FVC, Predicted MVV และ HRR ในกลุ่มทดลองและกลุ่มควบคุม สรุปได้ว่าการฝึกหายใจแบบช้าโดยใช้กล้ามเนื้อกระบังลมเป็นระยะเวลา 4 สัปดาห์ มีผลต่อการขยายตัวของทรวงอกเพิ่มขึ้น โดยไม่มีผลต่อการเปลี่ยนแปลงสมรรถภาพปอด และความสมดุลของระบบประสาทอัตโนมัติ ในผู้ที่เป็นโรคอ้วนช่วงวัยผู้ใหญ่ตอนต้น
เอกสารอ้างอิง
Ansari, S., Haboubi, H., & Haboubi, N. (2020). Adult obesity complications: Challenges and clinical impact. Therapeutic Advances in Endocrinology and Metabolism, 11, 204201882093495. https://doi.org/10.1177/2042018820934955
Barbosa Lins, T. C., Valente, L. M., Sobral Filho, D. C., & Barbosa e Silva, O. (2015). Relation between heart rate recovery after exercise testing and body mass index. Revista Portuguesa de Cardiologia, 34(1), 27-33. https://doi.org/10.1016/j.repc.2014.07.006
Barcelar J. dem., et al. (2014). The expansion of the pulmonary rib cage during breath stacking is influenced by age in obese women. PLoS One, 9(11), e110959. https://doi.org/10.1371/journal.pone.0110959
Bhaskaran, K., Dos-Santos-Silva, I., Leon, D. A., Douglas, I. J., & Smeeth, L. (2018). Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol, 6(12), 944-953. https://doi.org/10.1016/s2213-8587(18)30288-2
Chlif, M., Keochkerian, D., Choquet, D., Vaidie, A., & Ahmaidi, S. (2009). Effects of obesity on breathing pattern, ventilatory neural drive and mechanics. Respiratory Physiology & Neurobiology, 168(3), 198-202. https://doi.org/10.1016/j.resp.2009.06.012
Dixon, A. E., & Peters, U. (2018). The effect of obesity on lung function. Expert Review of Respiratory Medicine, 12(9), 755-767. https://doi.org/10.1080/17476348.2018.1506331
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/bf03193146
Gallagher, D., et al. (2000). Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. The American Journal of Clinical Nutrition, 72(3), 694-701. https://doi.org/10.1093/ajcn/72.3.694
González, Y., et al., (2022). Pulmonary function test in obese patients. European Respiratory Journal, 60(suppl 66), 3060. https://doi.org/10.1183/13993003.congress-2022.3060
Hirakawa, Y., et al. (2016). The impact of body mass index on the associations of lipids with the risk of coronary heart disease in the Asia Pacific region. Preventive Medicine Reports, 3, 79-82. https://doi.org/10.1016/j.pmedr.2015.12.012
Hough. (2014). Physiotherapy in Respiratory and Cardiac Care: A problem-solving approach to respiratory and cardiac management (2 ed.). Oxford Singular Publishing Group.
Jerath, R., Edry, J. W., Barnes, V. A., & Jerath, V. (2006). Physiology of long pranayamic breathing: Neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Medical Hypotheses, 67(3), 566-571. https://doi.org/10.1016/j.mehy.2006.02.042
Kinlen, D., Cody, D., & O'Shea, D. (2018). Complications of obesity. QJM: An International Journal of Medicine, 111(7), 437-443. https://doi.org/10.1093/qjmed/hcx152
Mafort, T. T., Rufino, R., Costa, C. H., & Lopes, A. J. (2016). Obesity: Systemic and pulmonary complications, biochemical abnormalities, and impairment of lung function. Multidisciplinary Respiratory Medicine, 11, 28. https://doi.org/10.1186/s40248-016-0066-z
Mehari, A., et al. (2015). Obesity and Pulmonary Function in African Americans. PLoS One, 10(10), e0140610. https://doi.org/10.1371/journal.pone.0140610
Melo, L. C., Silva, M. A., & Calles, A. C. (2014). Obesity and lung function: A systematic review. Einstein (Sao Paulo), 12(1), 120-125. https://doi.org/10.1590/s1679-45082014rw2691
Mendonça, J., Pereira, H., Xará, D., Santos, A., & Abelha, F. J. (2014). Obese patients: Respiratory complications in the post-anesthesia care unit. Revista Portuguesa de Pneumologia, 20(1), 12-19. https://doi.org/10.1016/j.rppneu.2013.04.002
Olsén, M. F., Lönroth, H., & Bake, B. (1999). Effects of breathing exercises on breathing patterns in obese and non-obese subjects. Clinical Physiology and Biochemistry, 19(3), 251-257. https://doi.org/10.1046/j.1365-2281.1999.00167.x
Pal, G. K., Velkumary, S., & Madanmohan. (2004). Effect of short-term practice of breathing exercises on autonomic functions in normal human volunteers. Indian Journal of Medical Research, 120(2), 115-121.
Paprika, D., Gingl, Z., Rudas, L., & Zöllei, E. (2014). Hemodynamic effects of slow breathing: Does the pattern matter beyond the rate? Acta Physiologica Hungarica, 101(3), 273-281. https://doi.org/10.1556/aphysiol.101.2014.3.2
Shah, N. M., & Kaltsakas, G. (2023). Respiratory complications of obesity: From early changes to respiratory failure. Breathe (Sheff), 19(1), 220263. https://doi.org/10.1183/20734735.0263-2022
Zammit, C., Liddicoat, H., Moonsie, I., & Makker, H. (2010). Obesity and respiratory diseases. International Journal of General Medicine, 3, 335-343. https://doi.org/10.2147/ijgm.s11926
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 วารสารวิจัยการพยาบาลและการสาธารณสุข

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
1. บทความหรือข้อคิดเห็นใด ๆ ที่ปรากฏในวารสารวิจัยการพยาบาลและการสาธารณสุข ที่เป็นวรรณกรรมของผู้เขียน บรรณาธิการไม่จำเป็นต้องเห็นด้วย
2. บทความที่ได้รับการตีพิมพ์ถือเป็นลิขสิทธิ์ของ วารสารวิจัยการพยาบาลและการสาธารณสุข




