
Bilateral Third Nerve Palsies Secondary to Pituitary Apoplexy: A Case Report
DOI:
https://doi.org/10.33165/rmj.2026.e273522Keywords:
Third cranial nerve palsy, Pituitary apoplexy, Pupil involvementAbstract
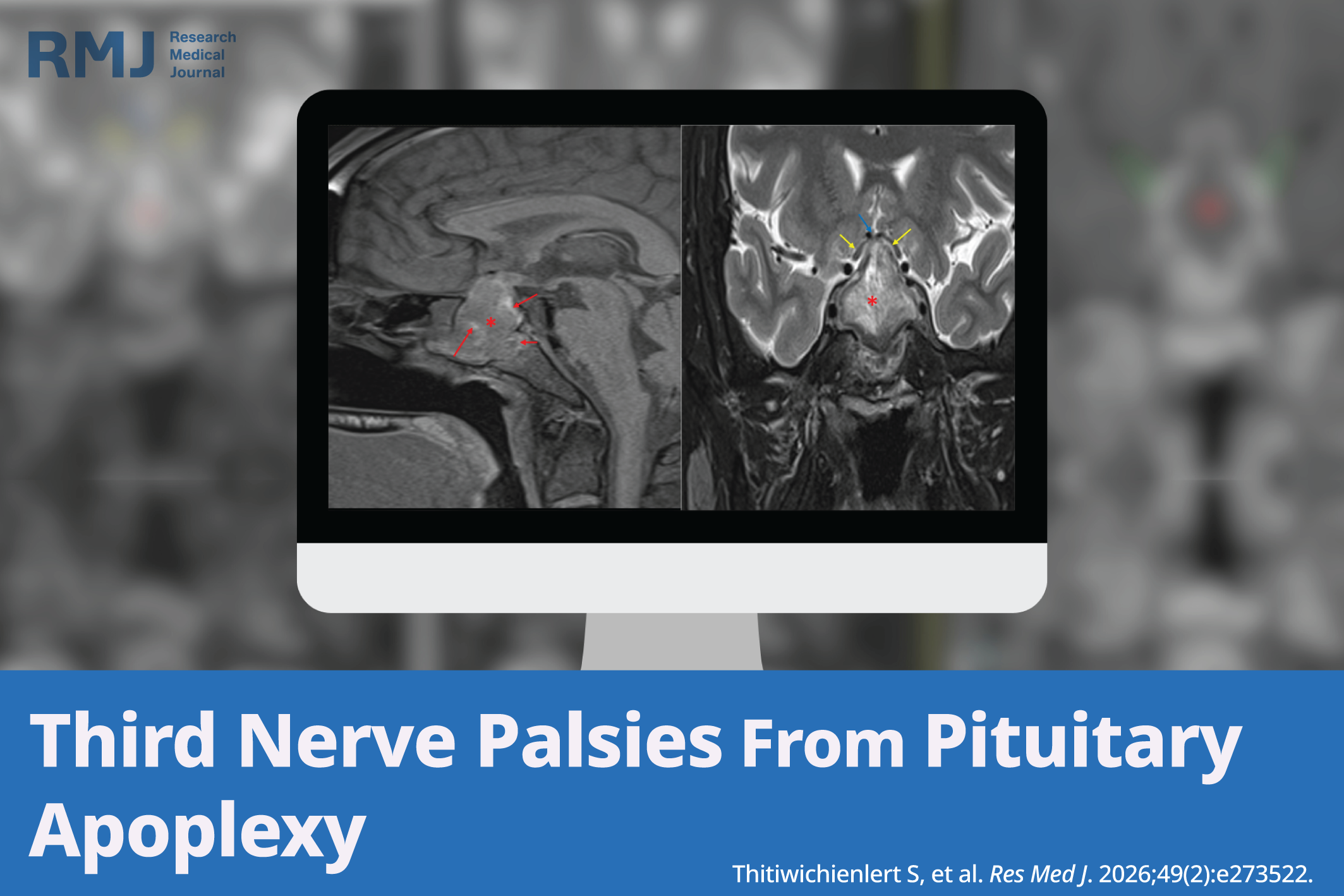
Background: Bilateral third cranial nerve palsies resulting from pituitary apoplexy with bilateral lateral expansion compressing bilateral third cranial nerves at the cavernous sinuses walls are uncommon.
Case Presentation: A 31-year-old healthy male complained of an acute severe headache, bilateral ptosis, and binocular horizontal diplopia for about 4 days. Eye examinations revealed incomplete ptosis, partial limitation of supraduction, infraduction, complete limitation of adduction, and dilated pupils in both eyes associated with bitemporal hemianopia. A brain computerized tomography (CT) scan with contrast revealed an intra- and suprasellar pituitary mass. Brain magnetic resonance imaging (MRI) reported a heterogenous mass measuring 3.0 × 3.1 × 3.8 cm involving the sphenoid sinus, sella turcica, and suprasellar cistern. Hormonal workup revealed the first diagnosis of type 2 diabetes mellitus, hyperprolactinemia, central hypothyroidism, and hypogonadotropic hypogonadism. The patient received hormonal supplements and the tumor was successfully treated by endoscopic surgery. Pathological confirmation of pituitary hemorrhage was found. All ocular and neurological deficits were completely resolved within 6 months postsurgery. Follow-up MRIs at 3 months and 1 year showed no residual tumor; however, hypogonadotropic hypogonadism and postoperative diabetes insipidus persisted for 4 months.
Conclusions: Localization of the third cranial nerve palsy was significant in determining the possibility of a lesion and detecting an emergency condition causing potential life-threatening complications. Most cases of third cranial nerve palsy from pituitary tumors effect one side, but this case is unusual because it involved both sides, showing a rare pattern of tumor growth and compression.
References
Barkhoudarian G, Kelly DF. Pituitary apoplexy. Neurosurg Clin N Am. 2019;30(4):457-463. doi:10.1016/j.nec.2019.06.001
Iglesias P. Pituitary apoplexy: an updated review. J Clin Med. 2024;13(9):2508. doi:10.3390/jcm13092508
Kasem MA, Kassem M, Taha AN, Kamal Al-S. Ocular motility disorders: unusual presentation of pituitary adenoma. J Egypt Ophthalmol Soc. 2018;111(2):43-48. doi:10.4103/ejos.ejos_16_18
Rosso M, Ramaswamy S, Sucharew H, Vagal A, Anziska Y, Levine SR. Isolated third cranial nerve palsy in pituitary apoplexy: case report and systematic review. J Stroke Cerebrovasc Dis. 2021;30(9):105969. doi:10.1016/j.jstrokecerebrovasdis.2021.105969
Keane JR. Third nerve palsy: analysis of 1400 personally-examined inpatients. Can J Neurol Sci. 2010;37(5):662-670. doi:10.1017/s0317167100010866
Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135(1):23-28. doi:10.1001/jamaophthalmol.2016.4456
Chavez-Herrera VR, Campero Á, Ballesteros-Herrera D, et al. Microsurgical and illustrative anatomy of the cavernous sinus, middle fossa, and paraclival triangles: a straightforward, comprehensive review. Surg Radiol Anat. 2023;45(4):389-400. doi:10.1007/s00276-023-03105-y
Hou Q, Xu L, Yi J. Pituitary apoplexy presenting with oculomotor nerve palsy and headache as the initial symptoms: a case report. Clin Case Rep. 2025;13(2):e70178. doi:10.1002/ccr3.70178
Lau KK, Joshi SM, Ellamushi H, Afshar F. Isolated bilateral oculomotor nerve palsy in pituitary apoplexy: case report and review. Br J Neurosurg. 2007;21(4):399-402. doi:10.1080/02688690701480710
Komurcu HF, Ayberk G, Ozveren MF, Anlar O. Pituitary adenoma apoplexy presenting with bilateral third nerve palsy and bilateral proptosis: a case report. Med Princ Pract. 2012;21(3):285-287. doi:10.1159/000334783
Komshian SR, Saket R, Bakhadirov K. Pituitary apoplexy with bilateral oculomotor nerve palsy. Neurohospitalist. 2018;8(3):NP4-NP5. doi:10.1177/1941874418773923
Man BL, Fu YP. Pituitary apoplexy presenting with bilateral oculomotor nerve palsy. BMJ Case Rep. 2015;2015:bcr2015212049. doi:10.1136/bcr-2015-212049
Mamelak AN, Little AS, Gardner PA, et al. A prospective, multicenter, observational study of surgical vs nonsurgical management for pituitary apoplexy. J Clin Endocrinol Metab. 2024;109(2):e711-e725. doi:10.1210/clinem/dgad541
Rajasekaran S, Vanderpump M, Baldeweg S, et al. UK guidelines for the management of pituitary apoplexy. Clin Endocrinol. 2011;74(1):9-20. doi:10.1111/j.1365-2265.2010.03913.x
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 by the Author(s). Licensee RMJ.

This work is licensed under a Creative Commons Attribution 4.0 International License.











