
แนวทางการดูแลผู้ป่วยที่เป็นโรคเริมที่อวัยวะเพศ ที่โรงพยาบาลศิริราช
Article Sidebar
Main Article Content
บทคัดย่อ
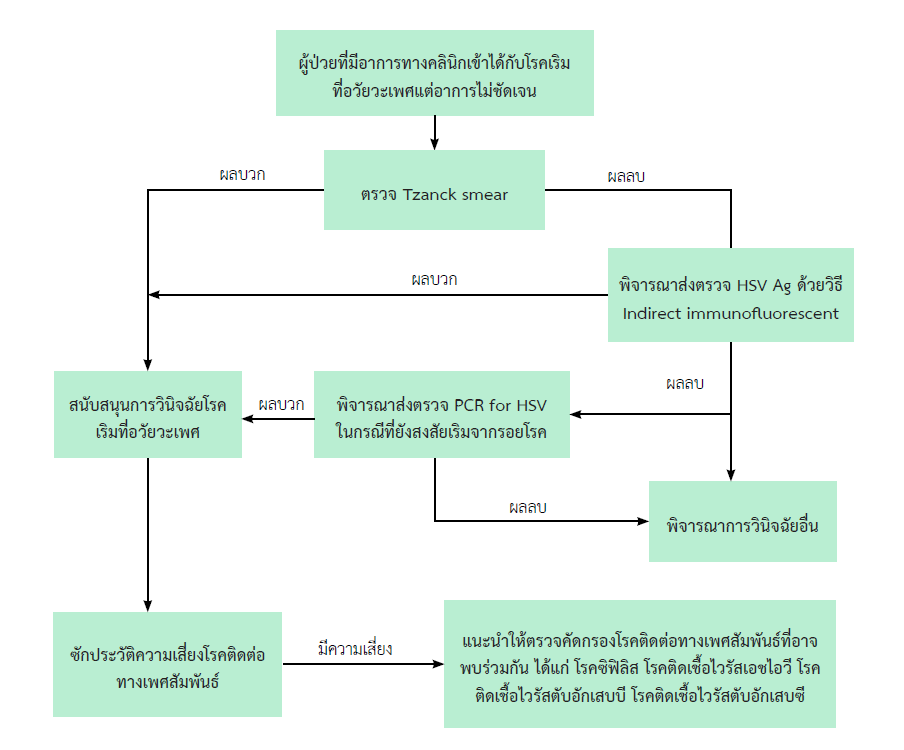
โรคเริมที่อวัยวะเพศ เป็นโรคติดต่อทางเพศสัมพันธ์ที่เกิดจากการติดเชื้อไวรัส Herpes simplex virus (HSV) ซึ่งแบ่งเป็น 2 ชนิด คือ HSV-1 และ HSV-2 โดย HSV-2 มักอาการรุนแรงและเกิดซ้ำบ่อยกว่า โรคเริมมีรอยโรคลักษณะเป็นตุ่มน้ำที่รวมเป็นกลุ่ม สามารถติดต่อผ่านการสัมผัสบริเวณตุ่มน้ำ เมื่อตุ่มน้ำแตกจะกลายเป็นแผลและเกิดการติดเชื้อแบคทีเรียซ้ำได้ ผู้ป่วยมักไม่มีอาการแม้ขณะมีการติดเชื้อไวรัส ทำให้ความชุกและการแพร่กระจายของโรคเกิดได้สูงมากขึ้น จากการเก็บข้อมูลของหน่วยตรวจโรคผิวหนังโรงพยาบาลศิริราชในผู้ป่วยที่มารับการรักษาที่คลินิกโรคติดต่อทางเพศสัมพันธ์ พบความชุกของโรคเริมที่อวัยวะเพศเพิ่มสูงขึ้นจาก ร้อยละ 15.4 เป็นร้อยละ 26.3 ในช่วงเวลา 5 ปีที่ผ่านมา การวินิจฉัยแยกโรคได้แก่ ซิฟิลิส แผลริมอ่อน และแผลที่อวัยวะเพศอื่น ๆ การวินิจฉัยหลักได้จากการซักประวัติและตรวจร่างกายจากรอยโรคที่จำเพาะ การส่งตรวจทางห้องปฏิบัติการเพิ่มเติมเพื่อสนับสนุนการวินิจฉัย ได้แก่ Tzanck smear ซึ่งนิยมใช้มากในโรงพยาบาลศิริราช เนื่องจากตรวจได้ง่ายและค่าใช้จ่ายต่ำ การตรวจหาแอนติเจนและการตรวจหาชิ้นส่วนพันธุกรรมของเชื้อในกรณีผู้ป่วยที่อาการไม่แน่ชัด นอกจากนี้การตรวจทางซีโรโลยี เช่น HSV IgG และ HSV IgM ก็มีส่วนช่วยในการพิจารณาการดูแลผู้ป่วยอย่างเหมาะสม การรักษาหลักในปัจจุบัน คือ ยาต้านไวรัส acyclovir, valacyclovir หรือ famciclovir ชนิดรับประทาน โดยแบ่งเป็นการรักษาผู้ป่วยที่ติดเชื้อโรคเริมที่อวัยวะเพศครั้งแรกและผู้ป่วยที่เกิดซ้ำ ในผู้ป่วยมีภูมิคุ้มกันบกพร่องหรือหญิงตั้งครรภ์อาจมีการปรับขนาดยาที่ต่างจากคนทั่วไป หากการติดเชื้อไวรัส HSV เกิดในหญิงตั้งครรภ์สามารถแพร่เชื้อไปยังทารกระหว่างการคลอดได้ การรักษาขึ้นอยู่กับระยะของโรคและอายุครรภ์ ซึ่งการติดเชื้อเริมครั้งแรกระหว่างการตั้งครรภ์ในไตรมาสที่ 3 นับว่าเป็นช่วงเวลาที่อันตรายมากที่สุด นอกจากนี้ ผู้ป่วยติดเชื้อโรคเริมทุกคนควรได้รับคำแนะนำในการตรวจหาโรคติดต่อทางเพศสัมพันธ์ชนิดอื่นด้วย เช่น เชื้อไวรัสเอชไอวี ซิฟิลิส ไวรัสตับอักเสบ เป็นต้น
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




เอกสารอ้างอิง
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187.
Leeyaphan C, Surawan TM, Chirachanakul P, Prasertworonun N, Punyaratabandhu P, Omcharoen V, et al. Clinical characteristics of hypertrophic herpes simplex genitalis and treatment outcomes of imiquimod: a retrospective observational study. International Journal of Infectious Diseases. 2015;33:165-70.
Chaiyabutr C JN, Apinuntham C, Leeyaphan C, Jiamton S. . Comparison of the Sensitivity and Specificity of Tzanck Smear and Immunofluorescence Assay for the Diagnosis of Cutaneous Herpes Simplex Virus and Varicella Zoster Virus Infections in a Real-life Clinical Setting Siriraj Med J. 2021;73(5):305-11.
Singh A, Preiksaitis J, Ferenczy A, Romanowski B. The laboratory diagnosis of herpes simplex virus infections. Can J Infect Dis Med Microbiol. 2005;16(2):92-8.
LeGoff J, Péré H, Bélec L. Diagnosis of genital herpes simplex virus infection in the clinical laboratory. Virol J. 2014;11:83-.
Glass N, Nelson HD, Huffman LH, editors. Screening for Genital Herpes Simplex : Brief Update for the U . S . Preventive Services Task Force2005.
M Hansgeorg, K Heinz. Neoplasias and Hyperplasia of Muscular and Neural Origin. Fitzpatrick’s Dermatology 9th ed. New York: McGraw-Hill Education.2019.
Chaweekulrat P, Leeyaphan C. Hypertrophic Herpes Simplex Infections: successful adjuvant treatment with topical imiquimod. Thai J Dermatol 2020;36(1):1-6.
Leeyaphan C, Nanchaipruek Y, Phinyo P. Therapeutic outcomes and prognostic factors in patients with hypertrophic herpes simplex infection treated with imiquimod: A systematic review and meta-analysis of individual patient data from case reports and case series. J Dermatol. 2022;49(9):879-86.
Samies N, James SH. Prevention and treatment of neonatal Herpes simplex virus. Antiviral Res.2020;176:104721
Amecian College of Obstetricians and Gynecologists. ACOG Practice Bulletin No.220: Management of genital herpes in pregnancy. Obstetrics&Gynecology. 2020;135:e193-e202
Foley E, Clarke E, Beckett VA, Harrison S, Pillai A, FitzGerald M, Owen P, Low-Beer N, Patel R. Green-top guideline No. 30: Management of genital herpes in pregnancy. https://www.rcog.org.uk/guidance/browse-all-guidance/other-guidelines-and-reports/management-of-genital-herpes-in-pregnancy/ (Accessed 6 September 2022)
