
บทบาทพยาบาลในการป้องกันและการจัดการผู้ป่วยที่มีภาวะเลือดออกในทางเดินอาหาร
Article Sidebar
Main Article Content
บทคัดย่อ
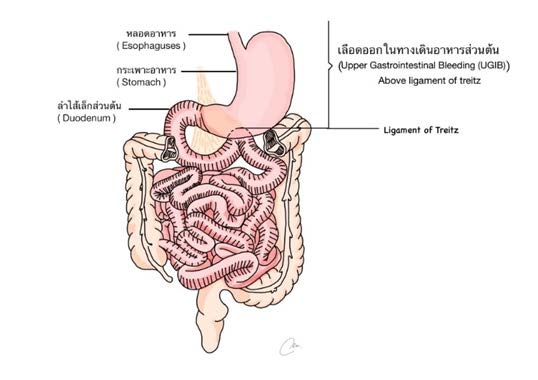
ภาวะเลือดออกในทางเดินอาหาร (Gastrointestinal bleeding) เป็นภาวะฉุกเฉินที่พบได้บ่อยในหอผู้ป่วยวิกฤต ภาวะแทรกซ้อนดังกล่าวส่งผลให้ผู้ป่วยมีการเสียเลือดจำนวนมากจนอาจทำให้เสียชีวิตได้ ผู้ป่วยบางรายต้องได้รับการรักษาในโรงพยาบาลนานขึ้น มีค่าใช้จ่ายในการรักษาเพิ่มขึ้น นอกจากนี้อาจกลายเป็นภาวะเจ็บป่วยเรื้อรังที่ทำให้ผู้ป่วยต้องเข้ารับการรักษาในโรงพยาบาลซ้ำ พยาบาลเป็นบุคคลที่มีบทบาทสำคัญในการป้องกันและให้การดูแลผู้ป่วยเบื้องต้น ดังนั้นจึงต้องมีความรู้ความเข้าใจพื้นฐานเกี่ยวกับภาวะเลือดออกในทางเดินอาหาร เช่น ความหมายของการเกิดเลือดออกในทางเดินอาหาร การจำแนกลักษณะความแตกต่างของพยาธิสภาพในแต่ละตำแหน่ง การประเมินความรุนแรงและพยาธิสรีรวิทยาที่เกิดจากการมีเลือดออกในทางเดินอาหาร ตลอดจนสามารถประเมินอาการและอาการแสดงของผู้ป่วยได้อย่างรวดเร็ว นอกจากนี้พยาบาลควรมีแนวทางการพยาบาลที่มีมาตรฐาน เพื่อเฝ้าระวังภาวะแทรกซ้อน การเตรียมผู้ป่วยในการส่งตรวจพิเศษต่าง ๆ การดูแลให้การพยาบาลขณะส่งตรวจและภายหลังการตรวจรักษา ดังนั้น การพยาบาลอย่างถูกต้องเหมาะสม รวดเร็ว
และมีองค์ความรู้ จะส่งผลให้เกิดความสำเร็จในการป้องกันภาวะฉุกเฉิน เพิ่มความปลอดภัยของผู้ป่วย และลดอัตราการเสียชีวิตของผู้ป่วยได้
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




เอกสารอ้างอิง
Zheng NS, Tsay C, Shung D, Laine L. Trends in characteristics, management, and outcomes of patients presenting with gastrointestinal bleeding to emergency departments in the United States from 2006 to 2019. Aliment Pharmacol Ther. 2022;56(11-12):1543-55.
Kamboj AK, Hoversten P, Leggett CL. Upper Gastrointestinal Bleeding: Etiologies and Management. Mayo Clin Proc. 2019;94(4):697-703.
Feinman M, Haut ER. Upper gastrointestinal bleeding. Surg Clin North Am. 2014;94(1):43-53.
Edelman DA, Sugawa C. Lower gastrointestinal bleeding: a review. Surg Endosc. 2007;21(4):514-20.
Costable NJ, Greenwald DA. Upper Gastrointestinal Bleeding. Clin Geriatr Med. 2021;37(1):155-72.
Oakland K. Changing epidemiology and etiology of upper and lower gastrointestinal bleeding. Best Pract Res Clin Gastroenterol. 2019;42-43:101610.
Tokar JL, Higa JT. Acute Gastrointestinal Bleeding. Ann Intern Med. 2022;175(2):ITC17-ITC32.
Kim JS, Kim BW, Kim DH, Park CH, Lee H, Joo MK, et al. Guidelines for Non-variceal Upper Gastrointestinal Bleeding. Korean J Gastroenterol. 2020;75(6):322-32.
Wilkins T, Wheeler B, Carpenter M. Upper Gastrointestinal Bleeding in Adults: Evaluation and Management. Am Fam Physician. 2020;101(5):294-300.
Whitehurst BD. Lower Gastrointestinal Bleeding. Surg Clin North Am. 2018;98(5):1059-72.
Barkun AN, Almadi M, Kuipers EJ, Laine L, Sung J, Tse F, et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations from the International Consensus Group. Ann Intern Med. 2019 ;171(11):805-22.
Kamboj AK, Hoversten P, Leggett CL. Upper Gastrointestinal Bleeding: Etiologies and Management. Mayo Clin Proc. 2019;94(4):697-703.
Rex DK, Schoenfeld PS, Cohen J, Pike IM, Adler DG, Fennerty MB, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015;81(1):31-53.
Strate LL, Syngal S. Timing of colonoscopy: impact on length of hospital stay in patients with acute lower intestinal bleeding. Am J Gastroenterol 2003;98(2):317-22.
Gady JS, Reynolds H, Blum A. Selective arterial embolization for control of lower gastrointestinal bleeding: recommendations for a clinical management pathway. Curr Surg. 2003;60(3):344-7.
Loffroy R, Rao P, Ota S, Lin MD, Kwak BK, Geschwind JF. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol 2010;33(6):1088-100.
Gerson L, Kamal A. Cost-effectiveness analysis of management strategies for obscure GI bleeding. Gastrointest Endosc 2008;68(5):920-36.
Gillespie CJ, Sutherland AD, Mossop PJ, Woods RJ, Keck JO, Heriot AG. Mesenteric embolization for lower gastrointestinal bleeding. Dis Colon Rectum 2010;53(9):1258-64.
