
อุบัติการณ์และการจัดการของอาการยึกยือเหตุยาในผู้ป่วยจิตเวช : การศึกษาเชิงพรรณนาแบบย้อนหลังของโรงพยาบาลจิตเวชแห่งหนึ่ง
คำสำคัญ:
อาการยึกยือเหตุยา, โรคทางจิตเวช, ยาต้านโรคจิตบทคัดย่อ
ความเป็นมา: อาการยึกยือเหตุยาเป็นอาการไม่พึงประสงค์ที่สำคัญจากยาต้านโรคจิต
วัตถุประสงค์: เพื่อศึกษาอุบัติการณ์และการจัดการอาการยึกยือเหตุยาในผู้ป่วยโรคทางจิตเวช
วิธีวิจัย: ทำการศึกษาย้อนหลังโดยเก็บข้อมูลระหว่างวันที่ 1 ตุลาคม 2550 ถึง วันที่ 30 กันยายน 2560 จากเวชระเบียนผู้ป่วยของโรงพยาบาลจากผู้ที่ได้รับการวินิจฉัยอาการยึกยือเหตุยาที่มีรหัสวินิจฉัย 333.85 หรือ G24.01 หรือผู้ป่วยที่มีอาการที่เข้าได้กับอาการยึกยือเหตุยาแต่ยังไม่ได้รับการวินิจฉัย ทำการวิเคราะห์ข้อมูลโดยใช้สถิติเชิงพรรณนา
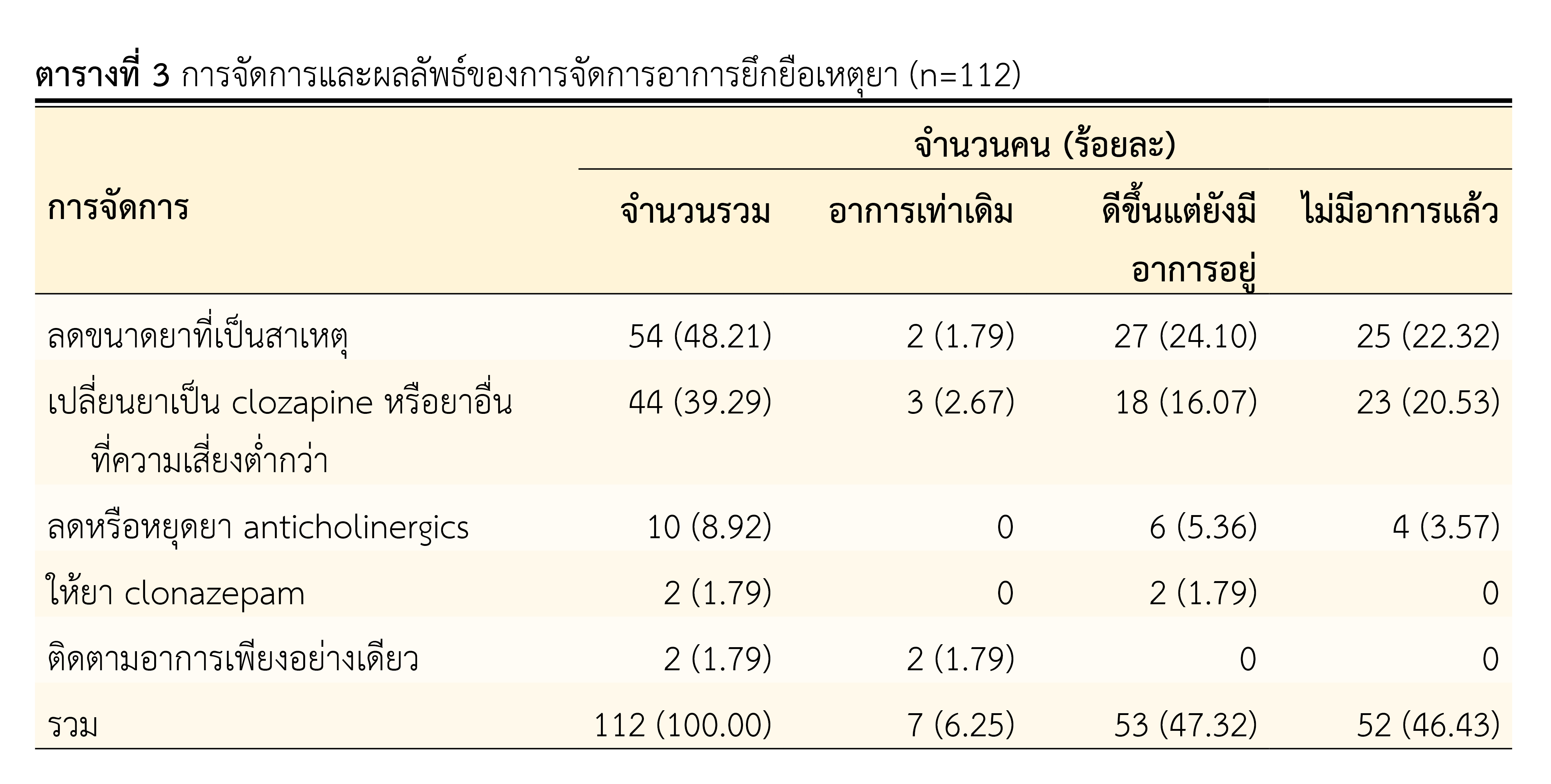
ผลการวิจัย: การศึกษานี้พบผู้ป่วยที่เกิดอาการยึกยือเหตุยา จำนวน 112 คน คิดเป็นอุบัติการณ์ร้อยละ 0.14 อายุเฉลี่ยของผู้ป่วยคือ 53 ปี ส่วนใหญ่เป็นเพศชาย ได้รับการวินิจฉัยโรคจิตเภท (F20-F29) มากที่สุด บริเวณที่เกิดอาการยึกยือเหตุยาที่พบมากที่สุด คือ รอบปาก จำนวน 105 คน คิดเป็นร้อยละ 72.41 สำหรับยาที่ทำให้เกิดอาการยึกยือเหตุยา พบว่ายาต้านโรคจิตกลุ่มเก่าเป็นสาเหตุมากที่สุดถึงร้อยละ 70.06 ยาที่มีรายงานมากที่สุด คือ Fluphenazine long-acting injection การจัดการอาการยึกยือเหตุยาส่วนใหญ่จัดการโดยการลดขนาดยาที่เป็นสาเหตุ รองลงมาคือการเปลี่ยนไปใช้ยา clozapine หรือยาอื่นที่ความเสี่ยงต่ำกว่า ซึ่งพบว่าผู้ป่วยส่วนใหญ่มีอาการลดลงหรือไม่มีอาการหลังจากได้รับการจัดการ
สรุปผล: อาการยึกยือเหตุยาพบอุบัติการณ์ร้อยละ 0.14 ส่วนใหญ่มาจากการใช้ยาต้านโรคจิตกลุ่มเก่าและเมื่อได้รับการจัดการผู้ป่วยมีอาการดีขึ้นหรืออาการหายไป
เอกสารอ้างอิง
Citrome L, Saklad SR. Revisiting tardive dyskinesia: focusing on the basics of identification and treatment. J Clin Psychiatry. 2020;81(2):TV18059AH3C. doi:10.4088/JCP.TV18059AH3C.
Waln O, Jankovic J. An update on tardive dyskinesia: from phenomenology to treatment. Tremor Other Hyperkinet Mov (NY). 2013;3:1-11. doi: 10.7916/D88P5Z71.
Lerner PP, Miodownik C, Lerner V. Tardive dyskinesia (syndrome): Current concept and modern approaches to its management. Psychiatry Clin Neurosci. 2015;69(6):321-34.
Jankelowitz SK. Treatment of neurolept-induced tardive dyskinesia. Neuropsychiatr Dis Treat. 2013;9:1371-80.
Bhidayasiri R, Fahn S, Weiner WJ, Gronseth GS, Sullivan KL, Zesiewicz TA. Evidence-based guideline: treatment of tardive syndromes: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;81(5):463-9.
Woods SW, Morgenstern H, Saksa JR, Walsh BC, Sullivan MC, Money R, et al. Incidence of tardive dyskinesia with atypical and conventional antipsychotic medications: Prospective cohort study. J Clin Psychiatry. 2010;71(4):463-74. doi:10.4088/JCP.07m03890yel.
Carbon M, Hsieh CH, Kane JM, Correll CU. Tardive dyskinesia prevalence in the period of second-generation antipsychotic use: a meta-analysis. J Clin Psychiatry. 2017;78(3):e264-e78. doi:10.4088/JCP.16r10832.
Lerner V, Miodownik C. Motor symptoms of schizophrenia: is tardive dyskinesia a symptom or side effect? A modern treatment. Curr Psychiatry Rep. 2011;13(4):295-304.
Keepers GA, Fochtmann LJ, Anzia JM, Benjamin S, Lyness JM, Mojtabai R, et al. The American Psychiatric Association Practice Guideline for the treatment of patients with schizophrenia. Am J Psychiatry. 2020;177(9):868-72.
Achalia RM, Chaturvedi SK, Desai G, Rao GN, Prakash O. Prevalence and risk factors associated with tardive dyskinesia among Indian patients with schizophrenia. Asian J Psychiatr. 2014;9:31-5.
Solmi M, Pigato G, Kane JM, Correll CU. Clinical risk factors for the development of tardive dyskinesia. J Neurol Sci. 2018;389:21-7.
Yassa R, Jeste DV. Gender differences in tardive dyskinesia: a critical review of the literature. Schizophr Bull. 1992;18(4):701-15.
Zhang XY, Chen DC, Qi LY, Wang F, Xiu MH, Chen S, et al. Gender differences in the prevalence, risk and clinical correlates of tardive dyskinesia in Chinese schizophrenia. Psychopharmacology (Berl). 2009;205(4):647-54.
Diehl A, Reinhard I, Schmitt A, Mann K, Gattaz WF. Does the degree of smoking effect the severity of tardive dyskinesia? A longitudinal clinical trial. Eur Psychiatry. 2009;24(1):33-40.
Carbon M, Kane JM, Leucht S, Correll CU. Tardive dyskinesia risk with first- and second-generation antipsychotics in comparative randomized controlled trials: a meta-analysis. World Psychiatry. 2018;17(3):330-40.
Waln O, Jankovic J. An update on tardive dyskinesia: from phenomenology to treatment. Tremor and other hyperkinetic movements (New York, NY). 2013;3:tre-03-161-4138-1. doi: 10.7916/D88P5Z71.
Bhidayasiri R, Jitkritsadakul O, Friedman JH, Fahn S. Updating the recommendations for treatment of tardive syndromes: a systematic review of new evidence and practical treatment algorithm. J Neurol Sci. 2018;389:67-75.
Owens DC. Tardive dyskinesia update: treatment and management. BJPsych Advances. 2019;25(2):78-89.
Gharabawi GM, Bossie CA, Lasser RA, Turkoz I, Rodriguez S, Chouinard G. Abnormal involuntary movement scale (AIMS) and extrapyramidal symptom rating scale (ESRS): cross-scale comparison in assessing tardive dyskinesia. Schizophr Res. 2005;77(2-3):119-28.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2022 สมาคมเภสัชกรรมโรงพยาบาล(ประเทศไทย)

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความในวารสารเภสัชกรรมโรงพยาบาลเผยแพร่ภายใต้เงื่อนไขของสัญญาอนุญาตครีเอทีฟคอมมอนส์ในรูปแบบที่ต้องอ้างอิงแหล่งที่มา - ห้ามใช้เพื่อการค้า - ห้ามแก้ไขดัดแปลง เวอร์ชั่น 4.0 (CC BY-NC-ND 4.0) สามารถแจกจ่ายและนำบทความไปใช้ประโยชน์เพื่อการศึกษาได้แต่ต้องระบุการอ้างอิงถึงบทความจากเว็บไซต์วารสารเภสัชกรรมโรงพยาบาล ไม่สามารถนำบทความไปใช้เพื่อการพาณิชย์ใด ๆ เว้นแต่ได้รับอนุญาตจากบรรณาธิการวารสารเภสัชกรรมโรงพยาบาล และกรณีมีการนำบทความไปเรียบเรียงใหม่ เปลี่ยนแปลงเนื้อหา หรือเสริมเติมแต่งเนื้อหาของบทความ ท่านไม่สามารถนำบทความที่ปรับแต่งไปเผยแพร่ได้ในทุกกรณี
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้แต่งแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้แต่งแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้แต่งแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้แต่ง ไม่เกี่ยวข้องกับกองบรรณาธิการ


