
ผลของยาต้านเอสจีแอลทีทูในการป้องกันการเสื่อมของไตในผู้ป่วยโรคไตเรื้อรัง
คำสำคัญ:
คานากลิโฟลซิน, ดาพากลิโฟลซิน, เอ็มพากลิโฟลซิน, ยาต้านเอสจีแอลทีทู, โรคไตเรื้อรังบทคัดย่อ
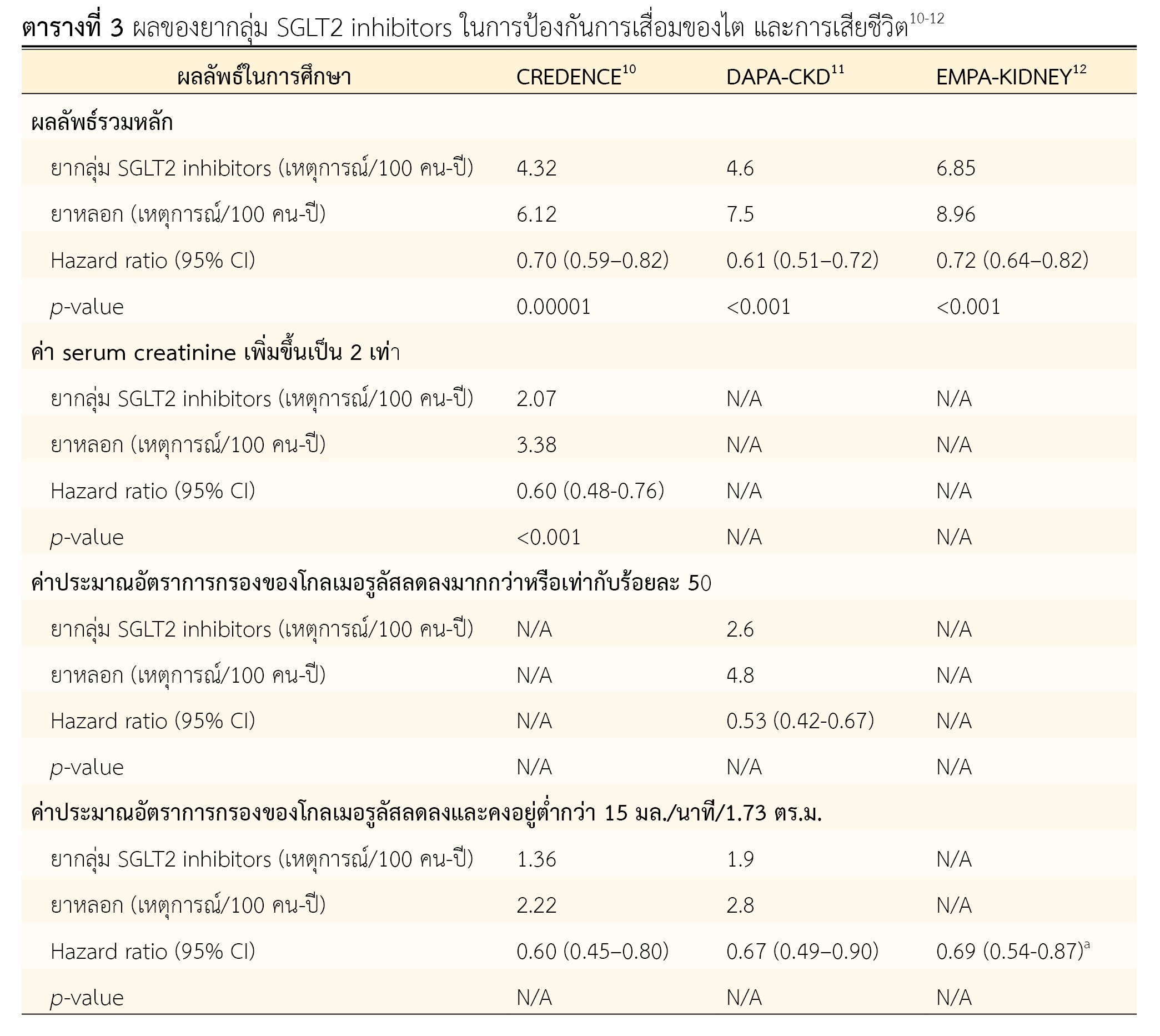
SGLT2 inhibitors เป็นยาลดน้ำตาลในเลือดออกฤทธิ์โดยยับยั้งโปรตีน sodium-glucose cotransporter type 2 ที่ท่อไตส่วนต้น เพิ่มการขจัดน้ำตาลออกทางปัสสาวะ ทำให้น้ำตาลในเลือดลดลง โดยมีการศึกษาแบบสุ่มและมีกลุ่มควบคุมในผู้ป่วยโรคไตเรื้อรังที่มีโปรตีนรั่วในปัสสาวะแสดงให้เห็นประโยชน์ของยาคานากลิโฟลซิน ดาพากลิโฟลซินและเอ็มพากลิโฟลซินที่ทำให้การดำเนินเข้าสู่โรคไตระยะสุดท้าย การเพิ่มขึ้นเป็นสองเท่าของครีอะตินีนในซีรั่ม การลดลงของค่าประมาณอัตราการกรองของโกลเมอรูลัส และการตายจากสาเหตุทางไตและสาเหตุทางหัวใจและหลอดเลือดลงได้ในภาพรวมประมาณร้อยละ 30 ในผู้ป่วยโรคไตเรื้อรังทั้งที่มีและไม่มีเบาหวาน ผู้ป่วยส่วนใหญ่ในการศึกษาเหล่านี้ยังคงมีโปรตีนรั่วในปัสสาวะในระดับปานกลางถึงรุนแรงแม้ได้รับยา renin-angiotensin system inhibitor ในขนาดสูงเท่าที่จะทนได้แล้ว และมีข้อควรระวังเกี่ยวกับการติดเชื้อราที่อวัยวะเพศ ภาวะของเหลวในร่างกายพร่อง และภาวะน้ำตาลในเลือดสูงร่วมกับเลือดเป็นกรดซึ่งควรได้รับการติดตามอย่างเหมาะสม
เอกสารอ้างอิง
Ehrenkranz JR, Lewis NG, Kahn CR, Roth J. Phlorizin: a review. Diabetes Metab Res Rev. 2005;21(1):31–8. doi: 10.1002/dmrr.532.
สมาคมโรคไตแห่งประเทศไทย. ข้อแนะนำเวชปฏิบัติการดูแลผู้ป่วยโรคไตเรื้อรัง ก่อนการบำบัดทดแทนไต พ.ศ. 2565 ฉบับปรับปรุงเพิ่มเติม. กรุงเทพฯ: ศรีเมืองการพิมพ์; 2565.
Rossing P, Caramori ML, Chan JC, Heerspink HJ, Hurst C, Khunti K, et al. Executive summary of the KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease: an update based on rapidly emerging new evidence. Kidney Int. 2022;102(5):990-9. doi: 10.1016/j.kint.2022.06.013.
Elsayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. The American Diabetes Association (ADA) pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl1):S140-57. doi: 10.2337/dc23-S009.
Neal B, Perkovic V, Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(21):2099. doi: 10.1056/NEJMc1712572.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28. doi: 10.1056/NEJMoa1504720.
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. doi: 10.1056/NEJMoa1911303.
Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089–98. doi: 10.1056/NEJMoa2206286.
Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–61. doi: 10.1056/NEJMoa2107038.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306. doi: 10.1056/NEJMoa1811744.
Heerspink HJL, Stefánsson B V., Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–46. doi: 10.1056/NEJMoa2024816.
Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117-27. doi: 10.1056/NEJMoa2204233.
Gerich JE. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: therapeutic implications. Diabet Med. 2010;27(2):136–42. doi: 10.1111/j.1464-5491.2009.02894.x.
Zeng Q, Zhou Q, Liu W, Wang Y, Xu X, Xu D. Mechanisms and perspectives of sodium-glucose co-transporter 2 inhibitors in heart failure. Front Cardiovasc Med. 2021;8:636152. doi: 10.3389/fcvm.2021.636152.
Scheen AJ. Pharmacodynamics, efficacy and safety of sodium-glucose co-transporter type 2 (SGLT2) inhibitors for the treatment of type 2 diabetes mellitus. Drugs. 2015;75(1):33–59. doi: 10.1007/s40265-014-0337-y.
Tsai KF, Chen YL, Chiou TTY, Chu TH, Li LC, Ng HY, et al. Emergence of SGLT2 inhibitors as powerful antioxidants in human diseases. Antioxidants (Basel). 2021;10(8):1166. doi: 10.3390/antiox10081166.
Miyata KN, Zhang SL, Chan JSD. The rationale and evidence for SGLT2 inhibitors as a treatment for nondiabetic glomerular disease. Glomerular Dis. 2021;1(1):21-33. doi: 10.1159/000513659.
Lytvyn Y, Bjornstad P, Udell JA, Lovshin JA, Cherney DZI. Sodium glucose cotransporter-2 inhibition in heart failure: potential mechanisms, clinical applications, and summary of clinical trials. Circulation. 2017;136(17):1643–58. doi: 10.1161/CIRCULATIONAHA.117.030012.
Cherney DZI, Charbonnel B, Cosentino F, Dagogo-Jack S, McGuire DK, Pratley R, et al. Effects of ertugliflozin on kidney composite outcomes, renal function and albuminuria in patients with type 2 diabetes mellitus: an analysis from the randomised VERTIS CV trial. Diabetologia. 2021;64(6):1256–67. doi: 10.1007/s00125-021-05407-5.
McGill JB, Subramanian S. Safety of sodium-glucose co-transporter 2 inhibitors. Am J Cardiol. 2019;132(10 Suppl):S49-57. doi: 10.1016/j.amjmed.2019.08.006.
Inzucchi SE, Iliev H, Pfarr E, Zinman B. Empagliflozin and assessment of lower-limb amputations in the EMPA-REG OUTCOME trial. Diabetes Care. 2018;41(1):e4-5. doi: 10.2337/dc17-1551.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 สมาคมเภสัชกรรมโรงพยาบาล(ประเทศไทย)

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความในวารสารเภสัชกรรมโรงพยาบาลเผยแพร่ภายใต้เงื่อนไขของสัญญาอนุญาตครีเอทีฟคอมมอนส์ในรูปแบบที่ต้องอ้างอิงแหล่งที่มา - ห้ามใช้เพื่อการค้า - ห้ามแก้ไขดัดแปลง เวอร์ชั่น 4.0 (CC BY-NC-ND 4.0) สามารถแจกจ่ายและนำบทความไปใช้ประโยชน์เพื่อการศึกษาได้แต่ต้องระบุการอ้างอิงถึงบทความจากเว็บไซต์วารสารเภสัชกรรมโรงพยาบาล ไม่สามารถนำบทความไปใช้เพื่อการพาณิชย์ใด ๆ เว้นแต่ได้รับอนุญาตจากบรรณาธิการวารสารเภสัชกรรมโรงพยาบาล และกรณีมีการนำบทความไปเรียบเรียงใหม่ เปลี่ยนแปลงเนื้อหา หรือเสริมเติมแต่งเนื้อหาของบทความ ท่านไม่สามารถนำบทความที่ปรับแต่งไปเผยแพร่ได้ในทุกกรณี
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้แต่งแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้แต่งแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้แต่งแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้แต่ง ไม่เกี่ยวข้องกับกองบรรณาธิการ


