
ยาชีววัตถุสำหรับรักษาโรคหืดชนิดรุนแรง
คำสำคัญ:
ยาชีววัตถุ, โรคหืดชนิดรุนแรงบทคัดย่อ
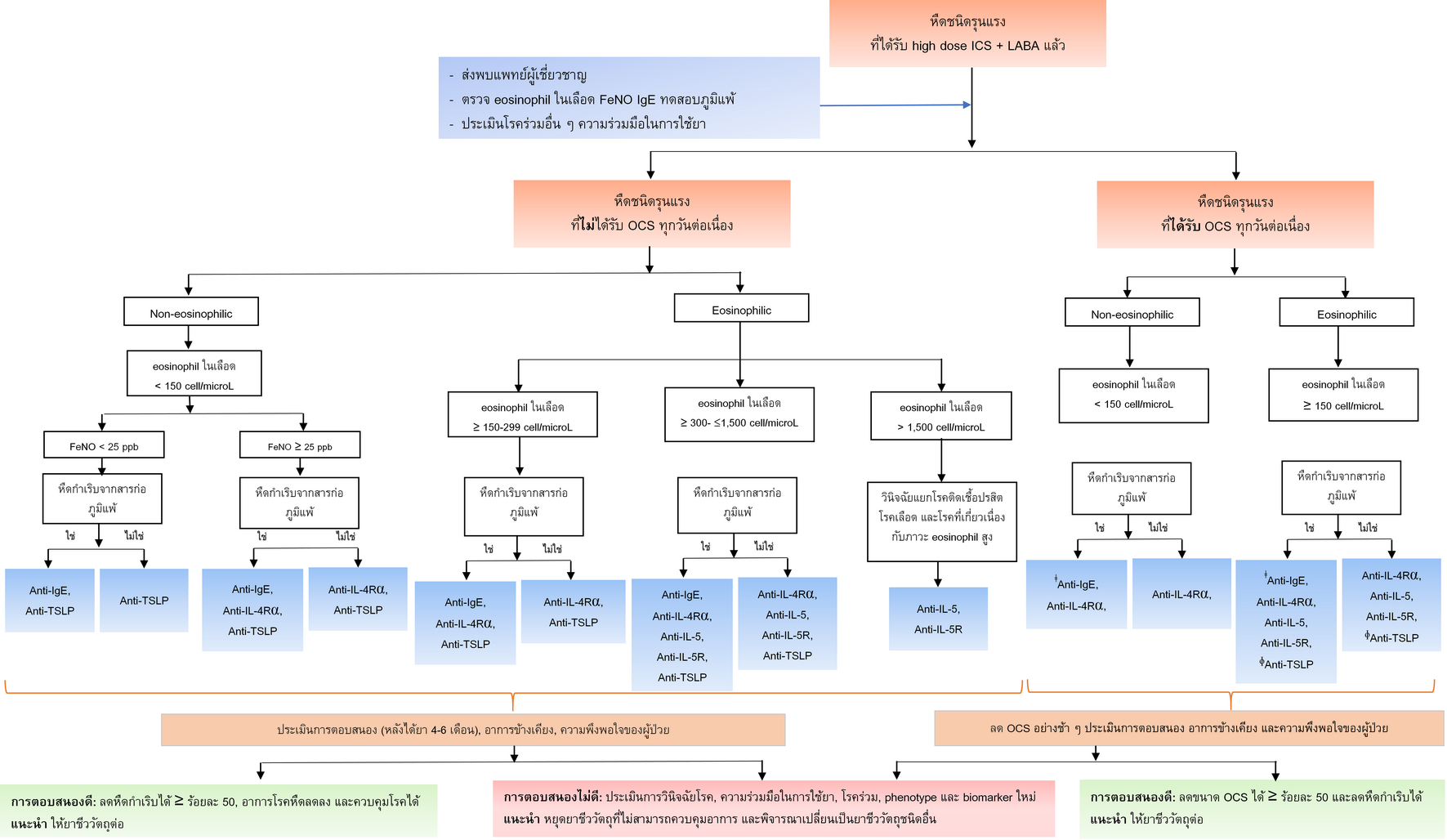
โรคหืดเป็นโรคเรื้อรังที่พบได้ในทุกกลุ่มอายุ ผู้ป่วยโรคหืดมีการอักเสบของหลอดลมเรื้อรัง หลอดลมไวต่อสิ่งกระตุ้นต่าง ๆ มากกว่าปกติ ส่งผลให้เกิดอาการทางเดินหายใจและหืดกำเริบ ผู้ป่วยที่เป็นโรคหืดชนิดรุนแรงมีการใช้คอร์ติโคสเตียรอยด์ชนิดพ่นสูดขนาดสูงร่วมกับยาควบคุมอาการ และอาจมีการใช้คอร์ติโคสเตียรอยด์ชนิดรับประทานเพื่อควบคุมโรค อย่างไรก็ตามการใช้คอร์ติโคสเตียรอยด์ชนิดรับประทานขนาดสูงมีความสัมพันธ์กับการเจ็บป่วยและอัตราตายที่เพิ่มขึ้น จากการศึกษาพยาธิสรีรวิทยาของการเกิดโรคหืดพบบทบาทของ type 2 inflammation และมีการตรวจตัวบ่งชี้ทางชีวภาพทำให้ทราบถึง endotype ของโรคหืดซึ่งส่งผลต่อการเลือกยารักษาแบบมุ่งเป้า รวมทั้งทำนายการตอบสนองต่อการรักษา ในปัจจุบันมี monoclonal antibody ซึ่งเป็นยาชีววัตถุสำหรับรักษาโรคหืดชนิดรุนแรง ได้แก่ omalizumab ออกฤทธิ์ที่ IgE, mepolizumab และ reslizumab ออกฤทธิ์ที่ interleukin (IL)-5, benralizumab ออกฤทธิ์ที่ IL-5 receptor, dupilumab ออกฤทธิ์ที่ IL-4 receptor และ tezepelumab ออกฤทธิ์เป็น anti-thymic stromal lymphopoietin นอกจากนั้น ยังมียาชีววัตถุในอนาคตที่อยู่ระหว่างการศึกษาวิจัยเพื่อรักษาโรคหืดชนิดรุนแรง ในบทความนี้ได้ทำการทบทวนพยาธิสรีรวิทยาของการเกิดโรคหืดชนิดรุนแรง ลักษณะอาการทางคลินิก และลักษณะทางพยาธิสรีรวิทยาของโรค การตรวจตัวบ่งชี้ทางชีวภาพที่เกี่ยวข้อง และหลักการเลือกยาชีววัตถุให้เหมาะกับผู้ป่วยโรคหืดชนิดรุนแรง
เอกสารอ้างอิง
GINA. Global strategy for asthma management and prevention (2024 update) [Internet]. n.p.: Global Initiative for Asthma (GINA); 2024 [cited 2024 Jun 1]. Available from: https://ginasthma.org/wp-content/uploads/2024/05/GINA-2024-Strategy-Report-24_05_22_WMS.pdf
Varricchi G, Ferri S, Pepys J, Poto R, Spadaro G, Nappi E, et al. Biologics and airway remodeling in severe asthma. Allergy. 2022;77(12):3538-52. doi: 10.1111/all.15473.
Kuruvilla ME, Lee FE-H, Lee GB. Understanding asthma phenotypes, endotypes, and mechanisms of disease. Clin Rev Allery Immunol. 2019;56(2):219-33. doi: 10.1007/s12016-018-8712-1.
Shah PA, Brightling C. Biologics for severe asthma—Which, when and why? Respirology. 2023;28(8):709-21. doi: 10.1111/resp.14520.
Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. NEJM. 2022;386(2):157-71. doi: 10.1056/NEJMra2032506.
Kyriakopoulos C, Gogali A, Bartziokas K, Kostikas K. Identification and treatment of T2-low asthma in the era of biologics. ERJ Open Res. 2021;7(2):00309-2020. doi: 10.1183/23120541.00309-2020.
Runnstrom M, Pitner H, Xu J, Lee FE-H, Kuruvilla M. Utilizing predictive inflammatory markers for guiding the use of biologicals in severe asthma. J Inflamm Res. 2022;15:241-9. doi: 10.2147/JIR.S269297.
Pelaia C, Pelaia G, Crimi C, Maglio A, Stanziola AA, Calabrese C, et al. Novel biological therapies for severe asthma endotypes. Biomedicines. 2022;10(5):1064. doi: 10.3390/biomedicines10051064.
Ramírez-Jiménez F, Pavón-Romero GF, Velásquez-Rodríguez JM, López-Garza MI, Lazarini-Ruiz JF, Gutiérrez-Quiroz KV, et al. Biologic therapies for asthma and allergic disease: past, present, and future. Pharmaceuticals. 2023;16(2):270. doi: 10.3390/ph16020270.
Micromedex. Omalizumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025 [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com Subscription required to view
Micromedex. Mepolizumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025. [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com. Subscription required to view.
Micromedex. Reslizumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025. [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com. Subscription required to view.
Micromedex. Benralizumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025. [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com. Subscription required to view.
Micromedex. Dupilumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025. [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com. Subscription required to view.
Micromedex. Tezepelumab. In: Adverse reactions [Internet]. n.p.: Micromedex, Merative US L.P.; 2025. [cited 2025 Mar 16]. Available from: www.micromedexsolutions.com. Subscription required to view.
Pelaia C, Crimi C, Vatrella A, Tinello C, Terracciano R, Pelaia G. Molecular targets for biological therapies of severe asthma. Front Immunol. 2020;11:603312. doi: 10.3389/fimmu.2020.603312.
Neighbour H, Boulet LP, Lemiere C, Sehmi R, Leigh R, Sousa AR, et al. Safety and efficacy of an oral CCR 3 antagonist in patients with asthma and eosinophilic bronchitis: a randomized, placebo‐controlled clinical trial. Clin Exp Allery. 2014;44(4):508-16. doi: 10.1111/cea.12244.
Cahn A, Hodgson S, Wilson R, Robertson J, Watson J, Beerahee M, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of GSK2239633, a CC-chemokine receptor 4 antagonist, in healthy male subjects: results from an open-label and from a randomised study. BMC Pharmacol Toxicol. 2013;14:14.. doi: 10.1186/2050-6511-14-14.
Tominaga SI, Ohta S, Tago K. Soluble form of the ST2 gene product exhibits growth promoting activity in NIH-3T3 cells. Biochem Biophys Rep. 2015;5:8-15. doi: 10.1016/j.bbrep.2015.11.020.
Calderon AA, Dimond C, Choy DF, Pappu R, Grimbaldeston MA, Mohan D, et al. Targeting interleukin-33 and thymic stromal lymphopoietin pathways for novel pulmonary therapeutics in asthma and COPD. Eur Respir Rev. 2023;32(167):220144. doi: 10.1183/16000617.0144-2022.
Kao CC, Parulekar AD. Spotlight on fevipiprant and its potential in the treatment of asthma: evidence to date. J Asthma Allergy. 2019;12:1-5. doi: 10.2147/JAA.S167973.
Brightling CE, Gaga M, Inoue H, Li J, Maspero J, Wenzel S, et al. Effectiveness of fevipiprant in reducing exacerbations in patients with severe asthma (LUSTER-1 and LUSTER-2): two phase 3 randomised controlled trials. Lancet Respir Med. 2021;9(1):43-56. doi: 10.1016/S2213-2600(20)30412-4.
Castro M, Kerwin E, Miller D, Pedinoff A, Sher L, Cardenas P, et al. Efficacy and safety of fevipiprant in patients with uncontrolled asthma: two replicate, phase 3, randomised, double-blind, placebo-controlled trials (ZEAL-1 and ZEAL-2). EClinicalMedicine. 2021;35: 100847. doi: 10.1016/j.eclinm.2021.100847.
AstraZeneca Clinical trials. Study to assess the efficacy and safety of MEDI3506 in adults with uncontrolled moderate-to-severe asthma (FRONTIER-3) [Internet]. n.p.: AstraZeneca Clinical Study Information Center, AstraZeneca; 2023 [cited 2025 Mar 16]. Available from: https://www.astrazenecaclinicaltrials.com/study/D9181C00001/
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2025 สมาคมเภสัชกรรมโรงพยาบาล(ประเทศไทย)

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความในวารสารเภสัชกรรมโรงพยาบาลเผยแพร่ภายใต้เงื่อนไขของสัญญาอนุญาตครีเอทีฟคอมมอนส์ในรูปแบบที่ต้องอ้างอิงแหล่งที่มา - ห้ามใช้เพื่อการค้า - ห้ามแก้ไขดัดแปลง เวอร์ชั่น 4.0 (CC BY-NC-ND 4.0) สามารถแจกจ่ายและนำบทความไปใช้ประโยชน์เพื่อการศึกษาได้แต่ต้องระบุการอ้างอิงถึงบทความจากเว็บไซต์วารสารเภสัชกรรมโรงพยาบาล ไม่สามารถนำบทความไปใช้เพื่อการพาณิชย์ใด ๆ เว้นแต่ได้รับอนุญาตจากบรรณาธิการวารสารเภสัชกรรมโรงพยาบาล และกรณีมีการนำบทความไปเรียบเรียงใหม่ เปลี่ยนแปลงเนื้อหา หรือเสริมเติมแต่งเนื้อหาของบทความ ท่านไม่สามารถนำบทความที่ปรับแต่งไปเผยแพร่ได้ในทุกกรณี
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้แต่งแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้แต่งแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้แต่งแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้แต่ง ไม่เกี่ยวข้องกับกองบรรณาธิการ


