Prevalence and Factors Associated with Superficial Cutaneous Fungal infections of Patients Treated at Public Hospitals in Trang Province
Keywords:
Superficial Cutaneous Fungal Infections, Hospital, Trang provinceAbstract
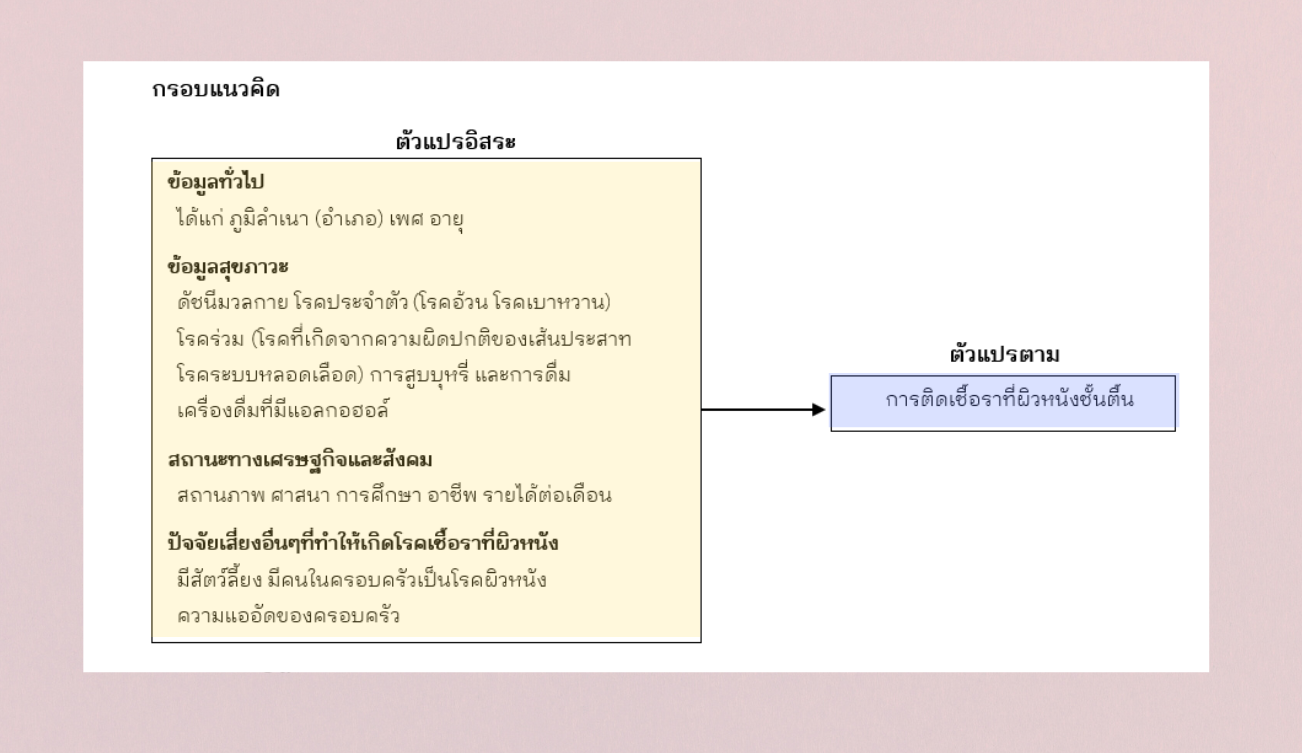
This cross-sectional study aimed to assess the prevalence and factors associated with superficial cutaneous fungal infections among patients treated at public hospitals in Trang Province. Data were collected using secondary data from the database of patients who visited hospitals under the Ministry of Public Health (MOPH) in Trang Province for the past 3 years, from January 1, 2021 to December 31, 2023, totaling 1,342 patients. The patients were diagnosed with superficial skin fungal infection and had a KOH preparation laboratory test result confirming the diagnosis. The data were analyzed using Multiple Logistic Regression statistics.
The results showed the prevalence of superficial skin fungal infections in patients admitted to hospitals under the MOPH, Trang Province was 33.2 percent, with Candida infection having the highest prevalence at 17.4 percent, followed by ringworm at 13.9 percent, and tinea versicolor at 1.9 percent, respectively. The district with the highest prevalence of superficial skin fungal infections was Hat Samran District at 58.18 percent, followed by Huai Yot District, Wang Wiset District, and Palian District, respectively. Factors significantly associated with superficial skin fungal infections were: 1) The patient's place of residence, i.e. Hat Samran District, Huai Yot District, Wang Wiset District, Palian District, and Mueang District had a higher risk of superficial skin fungal infections than Yan Ta Khao District, with OR values of 7.73, 5.60, 4.06, 2.95, and 2.15 times, respectively; 2) Marital status, where single patients were 1.49 times more likely to have superficial skin fungal infections than married patients, and patients with other statuses (divorced, widowed) were 1.86 times more likely to have superficial skin fungal infections than married patients; and 3) Smoking, where smokers were less likely to have superficial skin fungal infections than non-smokers, or had a 47% lower chance of having superficial skin fungal infections. For other factors, including education level, religion, occupation, and body mass index, no statistical significance was found (p-value > 0.05). Although occupation and body mass index were not statistically significant, it was found that patients with occupations as general employees, general laborers, farmers, or government officials had a significantly higher chance of getting superficial skin fungal infections than patients with occupations as merchants or self-employed (p-value < 0.05). Patients with a body mass index above normal had a significantly higher chance of getting superficial skin fungal infections than patients with normal body mass index (p-value < 0.05).The findings can be used to monitor, educate and plan for prevention of superficial skin fungal infections in risk groups, such as those residing in Hat Samran District, those who work as laborers or farmers, or those with a body mass index above normal, etc.
References
Ameen M. (2010). Epidemiology of superficial fungal infections. Clinics in dermatology., 28(2),
-201.
Baker LB. (2019) Physiology of sweat gland function: The roles of sweating and sweat
composition in human health.Temperature. 6(3):211-59.
Centers for Disease Control and Prevention. (2024). About Fungal Diseases.
https://www.cdc.gov/fungal/about/index.html#cdc_disease_basics_types-types
Chaiporn Wirotsaengarun. (2019). Histopathology of Cutaneous Fungal Infection. Faculty of
Medicine Naresuan University.http://www.med.nu.ac.th/dpMed/fileKnowledge/412_2023-
-14.pdf
Chayakulkeeree M, & Denning DW. (2017). Serious fungal infections in Thailand. European Journal
of Clinical Microbiology &Infectious Diseases. 36, 931-5.
GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. (2017, September 16).
Global, regional, and national incidence, prevalence, and years lived with disability for 328
diseases and injuries for 195 countries, a systematic analysis for the Global Burden of Disease
Study 2016. Lancet, 390
Institute for Health Metrics and Evaluation. (2018). Findings from the Global Burden of Disease
Study 2017.Institute of Dermatology Department of Medical Services, Ministry of Public
Health. (2023). Statistical report for fiscal year 2023. Institute of Dermatology. https://www.iod.go.th/
Kattaleeya Mekjaratsakul. (2017, October 25). Percutaneous absorption. Center for Continuing
Pharmacy Education.https://shorturl.asia/5tmcQ
Khodadadi H, et al. (2021), Zomorodian K, Nouraei H, Zareshahrabadi Z, Barzegar S, Zare MR, &
Pakshir K. Prevalence of superficial‐cutaneous fungal infections in Shiraz, Iran: A five‐year
retrospective study (2015–2019). Journal of Clinical Laboratory Analysis, 35(Suppl. 7),
e23850.
Phirun Mutsikapan. (2016). Common fungal diseases. Update from Infectious Disease Association
of Thailand. 11-14
Rasid S, Muthupalaniappen L, & Jamil A. (2020). A. Prevalence and factors associated with
cutaneous manifestations of type 2 diabetes mellitus. Clinical Diabetology, 9(Suppl. 6), 461-8.
Salinee Rojhiransakul, & Somyot Jaruwijitratana. (n.d.) Procedure and basic investigation in dermatology. Rama.Mahidol. https://www.rama.mahidol.ac.th/ramalaser/sites/default/files/public/pdf/course/Procedure.and.basic.investigation.in.dermatology.pdf
Sarker F, Akter T, Musa S, Bhuiyan AI, Khan MM, & Khanum H. (2021). Fungal Skin Diseases and
Related Factors in Outpatients of Three Tertiary Care Hospitals of Dhaka, an Urban City of
Bangladesh: Cross-Sectional Study. Biomed J Sci & Tech Res, 39(Suppl. 1), 30926-3.
Southern Regional hospital of Tropical Dermatology, Trang Province. (2023). Annual Report-2023.
Trangskin.https://www.trangskin.go.th/
Thai Healthy organization. (2019, February 21). How obesity cause skin damage. Thai Health
Promotion Foundation.https://www.thaihealth.or.th
Trang Provincial Administrative Organization. (2020). General information about Trang Province
Trangpao.https://www.trangpao.go.th/content/general
Ungpakorn R., Ishinkin N., &Zasshi G. (2005). Mycoses in Thailand: current concerns., 46(Suppl.
, 81-6.
Urban K, Chu S, Scheufele C, Giesey RL, Mehrmal S, Uppal P, & Delost GR. (2017). The global,
regional, and national burden of fungal skin diseases in 195 countries and territories: A cross-
sectional analysis from the Global Burden of Disease Study 2017. JAAD (Suppl. 2), 22-27. doi:
1016/j.jdin.2020.10.003. PMID: 34409349; PMCID: PMC8362308.
Walters KA. (2002, February 20). Dermatological and transdermal formulations. CRC Press.
Wasarin Natpracha. (2021). Common skin diseases and basic care to prevent disease spreading. Navavej.com https://navavej.com/articles_d/18855/Skin_diseases
Wu BY, Wu BJ, Lee SM, Sun HJ, Chang YT, & Lin MW. (2014). Prevalence and associated factors of
comorbid skin diseases in patients with schizophrenia: a clinical survey and national health
database study. General hospital psychiatry, 36(Suppl. 4),415-21.
Yuparat Srichuay, Woraphon Wechachapinan, & Phakamon Damrongkanapat. (2024, March 11).
The study of Dermatophytosis among service recipients at The Southern Regional hospital of
Tropical Dermatology, Trang Province, 2019 – 2023. Trangskin. https://www.trangskin.go.th/dermatophytosis/#
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Thai Journal of Public Health and Health Sciences

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความทุกบทความที่ได้รับการตีพิมพ์ถือเป็นลิขสิทธิ์ของ วารสารสาธารณสุข