
การพัฒนาและประเมินประสิทธิผลแนวปฏิบัติทางคลินิกในการป้องกันภาวะสับสนเฉียบพลันของผู้ป่วยวิกฤต หอผู้ป่วยอายุรกรรม 3 โรงพยาบาลลำปาง
คำสำคัญ:
แนวปฏิบัติทางคลินิก, การป้องกันภาวะสับสนเฉียบพลัน, ผู้ป่วยวิกฤตบทคัดย่อ
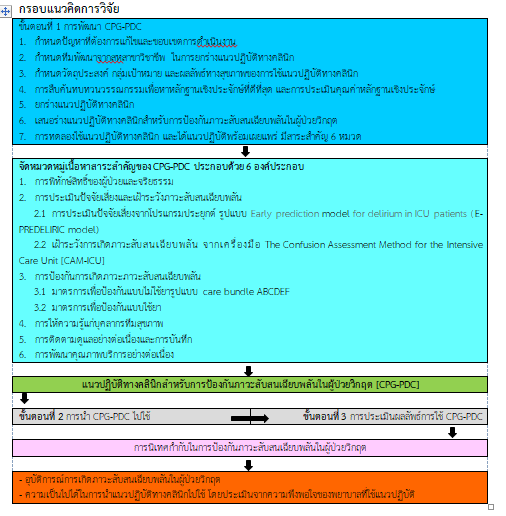
การวิจัยเชิงพัฒนานี้ มีวัตถุประสงค์เพื่อพัฒนาและประเมินประสิทธิผลแนวปฏิบัติทางคลินิกสำหรับการป้องกันภาวะสับสนเฉียบพลันในผู้ป่วยวิกฤตโรงพยาบาลลำปาง ดำเนินการตามกรอบแนวคิดของสภาวิจัยด้านการแพทย์และสุขภาพประเทศออสเตรเลีย คัดเลือกกลุ่มตัวอย่างแบบเจาะจง คือ ผู้ป่วยรู้สึกตัวดี สื่อสารได้ แบ่งออกเป็น 3 กลุ่มคือ 1) กลุ่มประชากรผู้พัฒนาแนวปฏิบัติทางคลินิกในการป้องกันภาวะสับสนเฉียบพลันของผู้ป่วยวิกฤต (CPG-PDC) 18 คน 2) กลุ่มตัวอย่างผู้ทดลองใช้ CPG-PDC 5 คน และ 3) กลุ่มตัวอย่างผู้ได้รับ CPG-PDC ดำเนินการระหว่างเดือนตุลาคม พ.ศ. 2560 – เมษายน พ.ศ. 2561 จำนวน 106 คน เครื่องมือที่ใช้ คือ CPG-PDC และแบบบันทึกอุบัติการณ์การเกิดภาวะสับสนเฉียบพลัน ข้อมูลทั่วไปใช้สถิติเชิงพรรณนา ร้อยละ ค่าเฉลี่ย ส่วนเบี่ยงเบนมาตรฐาน Independent t-test และ Multivariable risk difference regression
ผลการวิจัย พบว่า CPG-PDC มีสาระสำคัญ 6 หมวด คือ 1) การพิทักษ์สิทธิของผู้ป่วยและจริยธรรม 2) การประเมินปัจจัยเสี่ยงและเฝ้าระวังภาวะสับสนเฉียบพลัน โดยการประเมินปัจจัยเสี่ยงจากโปรแกรมประยุกต์ และจากเครื่องมือ (CAM-ICU) 3) การป้องกันภาวะสับสนเฉียบพลัน ใช้มาตรการรูปแบบไม่ใช้ยา Care bundle ABCDEF 4) การให้ความรู้แก่บุคลากรทีมสุขภาพ 5) การติดตามดูแลอย่างต่อเนื่องและการบันทึก และ 6) การพัฒนาคุณภาพบริการ เมื่อใช้ CPG-PDC จำนวน 106 ราย พบว่า มีอุบัติการณ์การเกิดภาวะสับสนเฉียบพลันลดลงเหลือเพียง 15 ราย (ร้อยละ 14.20) และระยะเวลาผู้ป่วยเกิดอุบัติการณ์การเกิดภาวะสับสนเฉียบพลัน เฉลี่ยลดลงเหลือ 0.9 เวรต่อราย สรุปการใช้ CPG-PDC ทำให้หน่วยงานมีการเฝ้าระวังและป้องกันอย่างเป็นระบบ สามารถลดอุบัติการณ์ และลดระยะเวลาการเกิดอุบัติการณ์การเกิดภาวะสับสนเฉียบพลันได้อย่างมีนัยสำคัญทางสถิติ
ดังนั้น แผนกผู้ป่วยวิกฤตควรให้ความสำคัญกับการจัดสิ่งแวดล้อมในการส่งเสริมการนอนหลับโดยการจัดชั่วโมงเงียบ โดยเฉพาะอย่างยิ่งการควบคุมระดับเสียงจากการทำกิจกรรมช่วยฟื้นคืนชีพ การทำหัตถการต่าง ๆ และควรนำผลการวิจัยเสนอต่อผู้บริหารเพื่อขยายผลไปยังหอผู้ป่วยอื่นรวมถึงการนำเอามาเป็นส่วนหนึ่งของงานประจำในหน่วยงานเพื่อให้เกิดการปฏิบัติที่ยั่งยืน
เอกสารอ้างอิง
Arend, E. & Christensen, M. (2009). Delirium in the intensive care unit: ฟ review. Nursing in Critical Care, 14(3), 145–154.
Bloom, B. S., Madaus, G. F., & Hastings, J. T. (1971). Handbook on formative and summative evaluation of student learning. New York: McGraw-Hill.
Boot, R. (2012). Delirium: a review of the nurse role in the intensive care unit. Intensive & Critical Care Nursing, 28(3), 185–189.
Bourne, R. S. (2008). Delirium and use of sedation agents in intensive care. Nursing in Critical Care, 13(4), 195-202.
Brummel, N. E., & Girard, T. D. (2013). Preventing delirium in the intensive care unit. Critical care Clinics, 29(1), 51-65.
Colombo, R., Corona, A., Praga, F., Minari, C., Giannotti, C., & Castelli, A., et al. (2012). A reorientation strategy for reducing delirium in the critically ill. Results of an interventional study. Minerva Anestesiologica, 78(9), 1026–1033.
Dennis, C. M., Lee, R., Woodard, E. K., Szalaj, J. J., & Walker, C. A. (2010). Benefits of quiet time for neuro-intensive care patients. The Journal of Neuroscience Nursing: Journal of the American Association of Neuroscience Nurses, 42(4), 217–224.
Desai, S., Chau, T., & George, L. (2013). Intensive care unit delirium. Critical Care Nursing Quarterly, 36(4), 370–389. Doungkaew, N. (2011). Effectiveness of implementing clinical practice guidelines for prevention of unplanned endotracheal extubations in medical intensive care unit, Lampang Hospital. Master of nursing science (Adult nursing) faculty of nursing, Chiang Mai University. (in Thai)
Environmental Protection Agency, Washington DC. (1974). Information on levels of environmental noise requisite to protect public health and welfare with an adequate margin of safety, Retrieved October 30, 2022 from https://www.nonoise.org/library/levels74/levels74.htm.
Fan, Y., Guo, Y., Li, Q., & Zhu, X. (2012). A review: nursing of intensive care unit delirium. The Journal of Neuroscience Nursing: Journal of the American Association of Neuroscience Nurses, 44(6), 307–316.
Hayhurst, C. J., Pandharipande, P. P., & Hughes, C. G. (2016). Intensive care unit delirium: a review of diagnosis, prevention, and treatment. Anesthesiology, 125(6), 1229–1241. doi: 10.1109/IEEESTD.2007.4299432.
Joanna Briggs Institute. (2013). JBI levels of evidence. Retrieved Jan 1, 2018 from https://jbi.global/sites/default/files/2019-05/JBI-Levels-of evidence_2014_0.pdf
King, J., & Gratrix, A. (2009). Delirium in intensive care. Continuing Education in Anaesthesia, Critical Care & Pain, 9(5), 144–147.
Konkani, A. & Oakley, B. (2012). Noise in hospital intensive care units - a critical review of a critical topic. Journal of Critical Care, 27(5), 522.e1-9.
Laohatanakom, S. (2014). Effectiveness of implementing clinical practice guidelines for prevention of delirium among critically ILL patients, medicial intensive care unit, Lampang hospital. Master of nursing science (Adult nursing) faculty of nursing, Chiang Mai University. (in Thai)
Laohatanakom, S. (2018). Clinical practice guidelines for the prevention of acute confusional states in Sub Intensive Care Unit. Lampang: Department of nursing, Lampang Hospital. (in Thai)
Linkaite, G., Riauka, M., Bunevičiute, I., & Vosylius, S. (2018). Evaluation of PRE-DELIRIC (PREdiction of DELIRium in ICu patients) delirium prediction model for the patients in the care unit. Acta Medica Lituanica, 25, 14-22.
Maldonado, J. R. (2008). Delirium in the acute care setting: Characteristics, diagnosis and treatment. Critical Care Clinics, 24(4), 657–722.
Maria, M. (2012). Delirium: a distressing and disturbing clinical event in a Intensive Care Unit. Health Science Journal, 6(4), 587-597.
Mistraletti, G., Pelosi, P., Mantovani, E. S., Berardino, M., & Gregoretti, C. (2012). Delirium: clinical approach and prevention, best practice & research. Clinical Anaesthesiology, 26(3), 311–326.
National Health and Medical Research Council. (1999). A guideline to the development, implementation and evaluation of clinical practice guideline. Canberra: Commonwealth Australia.
National Health and Medical Research Council. (2000). How to put the evidence into practice: Implementation and dissemination strategies. Canberra: Commonwealth Australia.
Pun, B. T., & Boehm, L. (2011). Delirium in the intensive care unit: Assessment and AACN Advanced Critical Care, 22(3), 225–237. https://doi.org/10.1097/NCI.0b013e318220c173
Rand, D., Lehman, B., & Shteynberg, A. (2007, June). Issues, models and solutions for triac modulated phase dimming of LED lamps. In 2007 IEEE Power Electronics Specialists Conference (pp. 1398-1404). IEEE.
Schiemann, A., Hadzidiakos, D., & Spies, C. (2011). Managing ICU delirium. Current Opinion in Critical Care, 17(2), 131–140.
Statistics of internal medicine wards registration III. (2017). Lampang: internal medicine wards. Lampang Hospital. (in Thai)
Tabet, N., & Howard, R. (2006). Prevention, diagnosis and treatment of delirium: Staff educational approaches. Expert Review of Neurotherapeutics, 6(5), 741–751.
Thongchai, C. (2005). Clinical practice guidelines development. The Thai Journal of Nursing Council, 20(2), 63-76.
Van Rompaey, B., Elseviers, M. M., Schuurmans, M. J., Shortridge-Baggett, L. M., Truijen, S., & Bossaert, L. (2009). Risk factors for delirium in intensive care patients: A prospective cohort study. Critical Care (London, England), 13(3), R77.
Van, R. B., Schuurmans, M. J., Shortridge-Baggett, L. M., Truijen, S., & Bossaert, L. (2008). Risk factors for intensive care delirium: A systematic review. Intensive & Critical Care Nursing, 24(2), 98–107.
Zomorodi, M., Topley, D., & McAnaw, M. (2012). Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU. Critical Care Research and Practice, 2012, 964547. doi: 10.1155/2012/964547
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 วิทยาลัยพยาบาลบรมราชชนนี นครศรีธรรมราช

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความที่ได้รับการตีพิมพ์เป็นลิขสิทธิ์ของ วิทยาลัยพยาบาลบรมราชชนนี นครศรีธรรมราช
ข้อความที่ปรากฏในบทความแต่ละเรื่องในวารสารวิชาการเล่มนี้เป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับวิทยาลัยพยาบาลบรมราชชนนี นครศรีธรรมราช และบุคคลากรท่านอื่น ๆ ในวิทยาลัยฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใดๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเองแต่ผู้เดียว



