
อาการแสดงทางคลินิก ระดับโปรแลคติน และการจัดการ ในผู้ป่วยที่มีภาวะโปรแลคตินในเลือดสูงจากยาจิตเวช
คำสำคัญ:
ระดับโปรแลคติน, ยาจิตเวช, ภาวะโปรแลคตินในเลือดสูง, การจัดการบทคัดย่อ
ความเป็นมา: ภาวะโปรแลคตินในเลือดสูงเป็นอาการไม่พึงประสงค์ที่พบได้บ่อยในผู้ป่วยจิตเวชที่ได้รับยาต้านโรคจิต
วัตถุประสงค์: เพื่อศึกษาอาการแสดงทางคลินิกและผลลัพธ์การจัดการภาวะโปรแลคตินในเลือดสูง
วิธีวิจัย: การศึกษาเชิงวิเคราะห์แบบภาคตัดขวางในผู้ป่วยโรคทางจิตเวชที่ได้รับการรักษาด้วยยาต้านโรคจิต และมีอาการแสดงของภาวะโปรแลคตินในเลือดสูงโดยทำการคัดกรองจากแบบสอบถามที่พัฒนาโดยผู้วิจัย กลุ่มตัวอย่างได้รับการวัดระดับโปรแลคตินในเลือดที่เริ่มต้นและหลังจากได้รับการจัดการ
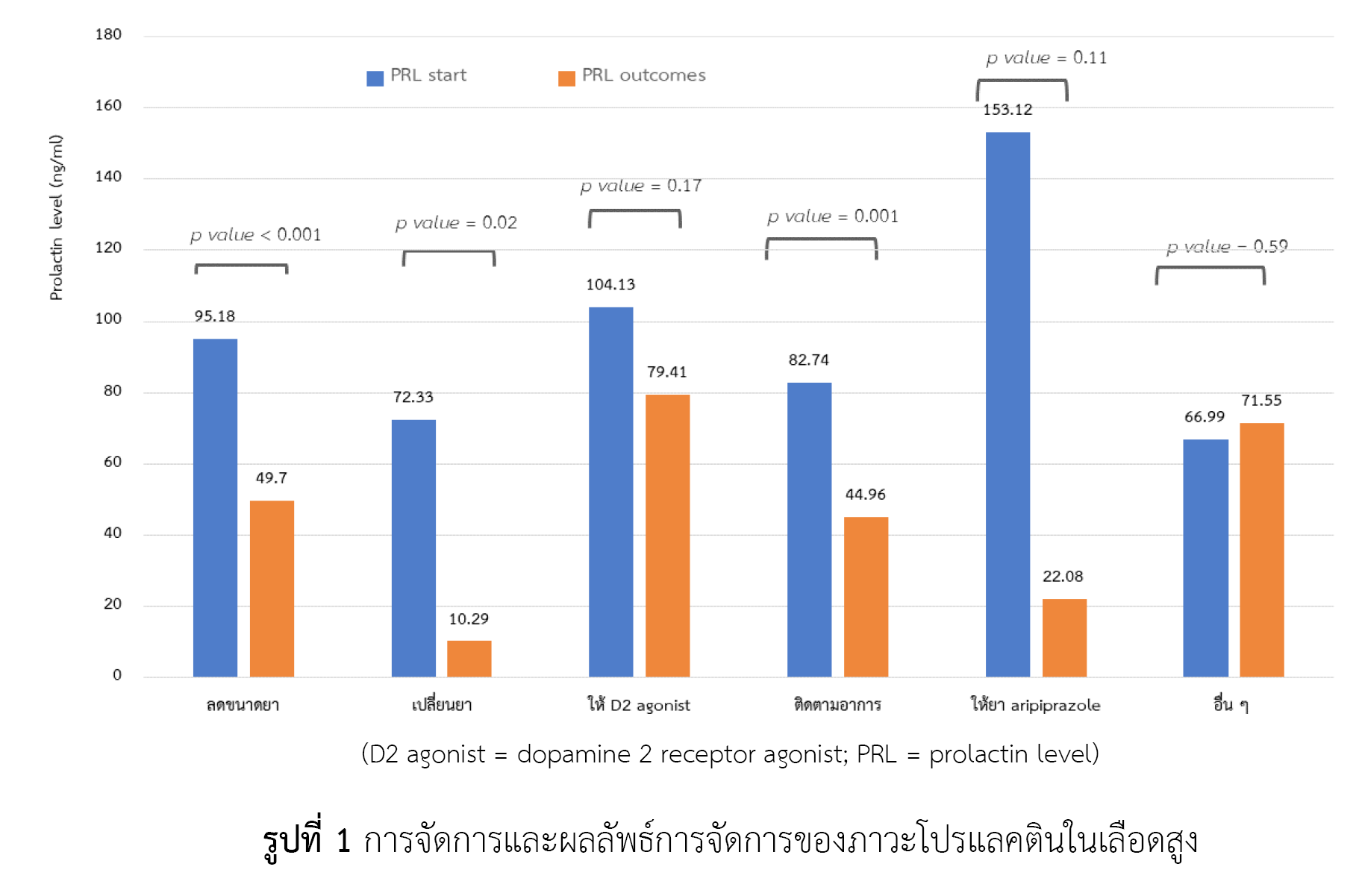
ผลการวิจัย: ผู้ป่วยที่เข้าร่วมการศึกษาจำนวน 127 ราย มีระดับโปรแลคตินในเลือดสูงจำนวน 109 ราย (ร้อยละ 85.83) อาการแสดงที่พบมากที่สุด คือ ประจำเดือนผิดปกติ จำนวน 84 ราย (ร้อยละ 77.06) พบค่าเฉลี่ยของระดับโปรแลคตินในเลือดมากที่สุดในกลุ่มผู้ป่วยที่ได้รับ amisulpride รองลงมาคือ paliperidone และยาต้านโรคจิตกลุ่มเก่าร่วมกับกลุ่มใหม่ ตามลำดับ การจัดการที่มีผลในการคงระดับโปรแลคตินในเลือดไม่ให้สูง ได้แก่ การลดขนาดยาที่เป็นสาเหตุ (p-value < 0.001) การเปลี่ยนยาเป็นยาที่คงระดับโปรแลคติน (p-value = 0.02) และการให้ยาขนาดเดิมและติดตามอาการ (p-value = 0.001)
สรุปผล: ผู้ป่วยจิตเวชที่มีอาการแสดงทางคลินิกที่เกี่ยวเนื่องกับโปรแลคตินสูงส่วนมากจะตรวจพบระดับโปรแลคตินสูง อาการแสดงที่พบมากที่สุดคือ ประจำเดือนผิดปกติ มีหลายวิธีการจัดการที่ลดระดับโปรแลคตินในเลือดได้อย่างมีนัยสำคัญ ควรมีการพัฒนาและวางแนวทางการติดตามและการจัดการภาวะนี้ในผู้ป่วยจิตเวชต่อไป
เอกสารอ้างอิง
Madhusoodanan S, Parida S, Jimenez C. Hyperprolactinemia associated with psychotropics--a review. Hum Psychopharmacol. 2010;25(4):281-97.
Fitzgerald P, Dinan TG. Prolactin and dopamine: What is the connection? A review article. J Psychopharmacol. 2008;22(2 Suppl):12-9.
Tewksbury A, Olander A. Management of antipsychotic-induced hyperprolactinemia. Ment Health Clin. 2016;6(4):185-90.
Bushe C, Shaw M, Peveler RC. A review of the association between antipsychotic use and hyperprolactinaemia. J Psychopharmacol. 2008;22(2 Suppl):46-55.
Byerly M, Suppes T, Tran QV, Baker RA. Clinical implications of antipsychotic-induced hyperprolactinemia in patients with schizophrenia spectrum or bipolar spectrum disorders: recent developments and current perspectives. J Clin Psychopharmacol. 2007;27(6):639-61.
Holt RI, Peveler RC. Antipsychotics and hyperprolactinaemia: mechanisms, consequences and management. Clin Endocrinol (Oxf). 2011;74(2):141-7.
Peuskens J, Pani L, Detraux J, De Hert M. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs. 2014;28(5):421-53.
Grigg J, Worsley R, Thew C, Gurvich C, Thomas N, Kulkarni J. Antipsychotic-induced hyperprolactinemia: synthesis of world-wide guidelines and integrated recommendations for assessment, management and future research. Psychopharmacology (Berl). 2017;234(22):3279-97.
Rusgis MM, Alabbasi AY, Nelson LA. Guidance on the treatment of antipsychotic-induced hyperprolactinemia when switching the antipsychotic is not an option. Am J Health Syst Pharm. 2021;78(10):862-71.
Dehelean L, Romosan AM, Papava I, Bredicean CA, Dumitrascu V, Ursoniu S, et al. Prolactin response to antipsychotics: an inpatient study. PLoS One. 2020;15(2):e0228648. doi: 10.1371/journal.pone.0228648.
Alosaimi FD, Fallata EO, Abalhassan M, Alhabbad A, Alzain N, Alhaddad B, et al. Prevalence and risk factors of hyperprolactinemia among patients with various psychiatric diagnoses and medications. Int J Psychiatry Clin Pract. 2018;22(4):274-81.
Walters J, Jones I. Clinical questions and uncertainty--prolactin measurement in patients with schizophrenia and bipolar disorder. J Psychopharmacol. 2008;22(2 Suppl):82-9.
Kelly DL, Conley RR. A randomized double-blind 12-week study of quetiapine, risperidone or fluphenazine on sexual functioning in people with schizophrenia. Psychoneuroendocrinology. 2006;31(3):340-6.
Roke Y, Buitelaar JK, Boot AM, Tenback D, van Harten PN. Risk of hyperprolactinemia and sexual side effects in males 10-20 years old diagnosed with autism spectrum disorders or disruptive behavior disorder and treated with risperidone. J Child Adolesc Psychopharmacol. 2012;22(6):432-9.
Bargiota SI, Bonotis KS, Messinis IE, Angelopoulos NV. The effects of antipsychotics on prolactin levels and women's menstruation. Schizophr Res Treatment. 2013;2013:502697. doi: 10.1155/2013/502697.
Glocker C, Grohmann R, Engel R, Seifert J, Bleich S, Stübner S, et al. Galactorrhea during antipsychotic treatment: results from AMSP, a drug surveillance program, between 1993 and 2015. Eur Arch Psychiatry Clin Neurosci. 2021;271(8):1425-35.
Rettenbacher MA, Hofer A, Ebenbichler C, Baumgartner S, Edlinger M, Engl J, et al. Prolactin levels and sexual adverse effects in patients with schizophrenia during antipsychotic treatment. J Clin Psychopharmacol. 2010;30(6):711-5.
Redman B, Kitchen C, Johnson KW, Bezwada P, Kelly DL. Levels of prolactin and testosterone and associated sexual dysfunction and breast abnormalities in men with schizophrenia treated with antipsychotic medications. J Psychiatr Res. 2021;143:50-3.
Kopecek M, Bares M, Svarc J, Dockery C, Horácek J. Hyperprolactinemia after low dose of amisulpride. Neuro Endocrinol Lett. 2004;25(6):419-22.
Skopek M, Manoj P. Hyperprolactinaemia during treatment with paliperidone. Australas Psychiatry. 2010;18(3):261-3.
Kearns AE, Goff DC, Hayden DL, Daniels GH. Risperidone-associated hyperprolactinemia. Endocr Pract. 2000;6(6):425-9.
Stojkovic M, Radmanovic B, Jovanovic M, Janjic V, Muric N, Ristic DI. Risperidone induced hyperprolactinemia: from basic to clinical studies. Front Psychiatry. 2022;13:874705. doi: 10.3389/fpsyt.2022.874705.
Gupta S, Lakshmanan DAM, Khastgir U, Nair R. Management of antipsychotic-induced hyperprolactinaemia. BJPsych Advances. 2017;23(4):278-86.
Labad J, Montalvo I, González-Rodríguez A, García-Rizo C, Crespo-Facorro B, Monreal JA, et al. Pharmacological treatment strategies for lowering prolactin in people with a psychotic disorder and hyperprolactinaemia: a systematic review and meta-analysis. Schizophr Res. 2020;222:88-96.
Navy H, Gardner K. Strategies for managing medication-induced hyperprolactinemia. Current Psychiatry. 2018;17(3):42-7.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2022 สมาคมเภสัชกรรมโรงพยาบาล(ประเทศไทย)

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความในวารสารเภสัชกรรมโรงพยาบาลเผยแพร่ภายใต้เงื่อนไขของสัญญาอนุญาตครีเอทีฟคอมมอนส์ในรูปแบบที่ต้องอ้างอิงแหล่งที่มา - ห้ามใช้เพื่อการค้า - ห้ามแก้ไขดัดแปลง เวอร์ชั่น 4.0 (CC BY-NC-ND 4.0) สามารถแจกจ่ายและนำบทความไปใช้ประโยชน์เพื่อการศึกษาได้แต่ต้องระบุการอ้างอิงถึงบทความจากเว็บไซต์วารสารเภสัชกรรมโรงพยาบาล ไม่สามารถนำบทความไปใช้เพื่อการพาณิชย์ใด ๆ เว้นแต่ได้รับอนุญาตจากบรรณาธิการวารสารเภสัชกรรมโรงพยาบาล และกรณีมีการนำบทความไปเรียบเรียงใหม่ เปลี่ยนแปลงเนื้อหา หรือเสริมเติมแต่งเนื้อหาของบทความ ท่านไม่สามารถนำบทความที่ปรับแต่งไปเผยแพร่ได้ในทุกกรณี
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้แต่งแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้แต่งแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้แต่งแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้แต่ง ไม่เกี่ยวข้องกับกองบรรณาธิการ


