
เภสัชบำบัดขั้นสูงของ tenecteplase ในการเป็นยาสลายลิ่มเลือดสำหรับรักษาผู้ป่วยโรคหลอดเลือดสมองขาดเลือดเฉียบพลัน
คำสำคัญ:
โรคหลอดเลือดสมอง, หลอดเลือดสมองขาดเลือดเฉียบพลัน, ยาสลายลิ่มเลือด, tenecteplaseบทคัดย่อ
ปัจจุบันการรักษาหลักในผู้ป่วยโรคหลอดเลือดสมองขาดเลือดเฉียบพลันจะเป็นการรักษาด้วย alteplase ซึ่งเป้าหมายการรักษาเพื่อลดความพิการ แต่พบข้อจำกัดของ alteplase คือมีอัตราการเกิดเลือดออกในสมองค่อนข้างสูงและยาออกฤทธิ์สั้น รวมถึงอัตราการได้รับ alteplase ของผู้ป่วยที่มีอาการภายใน 4.5 ชั่วโมง ในปัจจุบันมีเพียงร้อยละ 9.26 เท่านั้น จึงมีการพัฒนายาสลายลิ่มเลือด tenecteplase ขึ้นเพื่อลดข้อจำกัดดังกล่าว จากข้อมูลด้านเภสัชจลนศาสตร์และด้านเภสัชพลศาสตร์พบว่า tenecteplase มีค่าครึ่งชีวิตที่ยาวกว่า และมีความเฉพาะเจาะจงต่อไฟบรินมากกว่า alteplase ทำให้สามารถบริหารยาโดยการฉีดเข้าหลอดเลือดดำภายในระยะเวลาสั้นได้ ตามแนวทางการรักษา American Heart Association/American Stroke Association ค.ศ. 2019 ได้แนะนำการใช้ alteplase และ tenecteplase ซึ่งมีข้อมูลสนับสนุนตามหลักฐานเชิงประจักษ์พบว่า tenecteplase มีประสิทธิภาพสามารถลดความพิการและเกิดอาการข้างเคียงได้เช่นเดียวกับ alteplase แต่มีประสิทธิภาพดีกว่าในกลุ่มผู้ป่วยโรคหลอดเลือดสมองขาดเลือดที่มีการอุดตันหลอดเลือดขนาดใหญ่ ที่ต้องได้ทำหัตถการนำลิ่มเลือดออกผ่านทางสายสวน รวมถึงมีข้อมูลการศึกษาเพื่อนำไปใช้ในผู้ป่วยโรคหลอดเลือดสมองขาดเลือดเฉียบพลันอื่น ๆ ได้แก่ กลุ่มผู้ป่วยโรคหลอดเลือดสมองขาดเลือดภายใน 4.5 ชั่วโมงที่ไม่เข้าเกณฑ์การทำ mechanical thrombectomy กลุ่มผู้ป่วยโรคหลอดเลือดสมองขาดเลือดที่มีระยะเวลามากกว่า 4.5 ถึง 24 ชั่วโมง ปัจจุบันจึงมีการศึกษาของ tenecteplase ในกลุ่มผู้ป่วยโรคนี้มากขึ้นทั้งทางด้านประสิทธิภาพ ความปลอดภัย รวมถึงความคุ้มค่าด้านต้นทุนประสิทธิผล
เอกสารอ้างอิง
GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795-820. doi: 10.1016/S1474-4422(21)00252-0.
Berge E, Whiteley W, Audebert H, De Marchis GM, Fonseca AC, Padiglioni C, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I-LXII. doi: 10.1177/2396987321989865.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi: 10.1161/STR.0000000000000211.
National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581-7. doi: 10.1056/NEJM199512143332401.
Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317-29. doi: 10.1056/NEJMoa0804656.
American Academy of Emergency Medicine Work Group on Thrombolytic Therapy in Stroke. AAEM position statement on tPA: the use of intravenous thrombolytic therapy in the treatment of stroke [Internet]. Milwaukee (Wisconsin): American Academy of Emergency Medicine; 2002 [cited 2024 Jun 20]. Available from: https://www.aaem.org/statements/aaem-position-statement-on-tpa-the-use-of-intravenous-thrombolytic-therapy-in-the-treatment-of-stroke/
Logallo N, Kvistad CE, Nacu A, Thomassen L. Novel thrombolytics for acute ischemic stroke: challenges and opportunities. CNS Drugs. 2016;30(2):101-8. doi: 10.1007/s40263-015-0307-2.
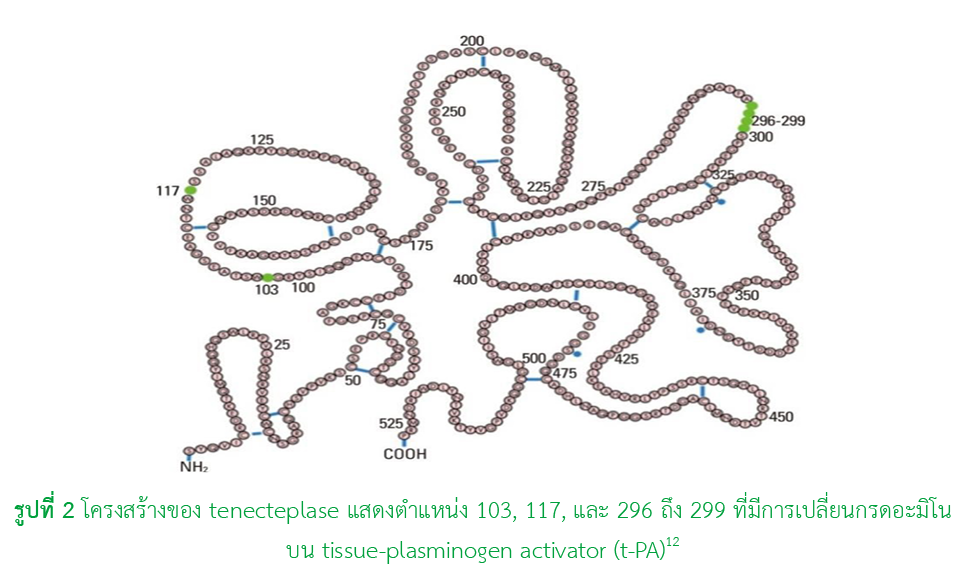
Baruah DB, Dash RN, Chaudhari MR, Kadam SS. Plasminogen activators: a comparison. Vascul Pharmacol. 2006;44(1):1-9. doi: 10.1016/j.vph.2005.09.003.
Wang L, Hao M, Wu N, Wu S, Fisher M, Xiong Y. Comprehensive review of tenecteplase for thrombolysis in acute ischemic stroke. J Am Heart Assoc. 2024;13(9):e031692. doi: 10.1161/JAHA.123.031692.
Cesarman-Maus G, Hajjar KA. Molecular mechanisms of fibrinolysis. Br J Haematol. 2005;129(3):307-21. doi: 10.1111/j.1365-2141.2005.05444.x.
Keyt BA, Paoni NF, Refino CJ, Berleau L, Nguyen H, Chow A, et al. A faster-acting and more potent form of tissue plasminogen activator. Proc Natl Acad Sci U S A. 1994;91(9):3670-4. doi: 10.1073/pnas.91.9.3670.
Bivard A, Lin L, Parsonsb MW. Review of stroke thrombolytics. J Stroke. 2013;15(2):90-8. doi: 10.5853/jos.2013.15.2.90.
Van De Werf F, Adgey J, Ardissino D, Armstrong PW, Aylward P, Barbash G, et al. Single-bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomised trial. Lancet. 1999;354(9180):716-22. doi: 10.1016/s0140-6736(99)07403-6.
Haley EC Jr., Thompson JL, Grotta JC, Lyden PD, Hemmen TG, Brown DL, et al. Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial. Stroke. 2010;41(4):707-11. doi: 10.1161/STROKEAHA.109.572040.
Logallo N, Novotny V, Assmus J, Kvistad CE, Alteheld L, Ronning OM, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. 2017;16(10):781-8. doi: 10.1016/S1474-4422(17)30253-3.
Campbell BCV, Mitchell PJ, Churilov L, Yassi N, Kleinig TJ, Dowling RJ, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK Part 2 randomized clinical trial. JAMA. 2020;323(13):1257-65. doi: 10.1001/jama.2020.1511.
Wang Y, Li S, Pan Y, Li H, Parsons MW, Campbell BCV, et al. Tenecteplase versus alteplase in acute ischaemic cerebrovascular events (TRACE-2): a phase 3, multicentre, open-label, randomised controlled, non-inferiority trial. Lancet. 2023;401(10377):645-54. doi: 10.1016/S0140-6736(22)02600-9.
Menon BK, Buck BH, Singh N, Deschaintre Y, Almekhlafi MA, Coutts SB, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet. 2022;400(10347):161-9. doi: 10.1016/S0140-6736(22)01054-6.
Muir KW, Ford GA, Ford I, Wardlaw JM, McConnachie A, Greenlaw N, et al. Tenecteplase versus alteplase for acute stroke within 4.5 h of onset (ATTEST-2): a randomised, parallel group, open-label trial. Lancet Neurol. 2024;23(11):1087–96. doi: 10.1016/S1474-4422(24)00377-6.
Yogendrakumar V, Churilov L, Mitchell PJ, Kleinig TJ, Yassi N, Thijs V, et al. Safety and efficacy of tenecteplase in older patients with large vessel occlusion: a pooled analysis of the EXTEND-IA TNK trials. Neurology. 2022;98(12):e1292-e301. doi: 10.1212/WNL.0000000000013302.
Coutts SB, Ankolekar S, Appireddy R, Arenillas JF, Assis Z, Bailey P, et al. Tenecteplase versus standard of care for minor ischaemic stroke with proven occlusion (TEMPO-2): a randomised, open label, phase 3 superiority trial. Lancet. 2024;403(10444):2597-605. doi: 10.1016/S0140-6736(24)00921-8
Albers GW, Jumaa M, Purdon B, Zaidi SF, Streib C, Shuaib A, et al. Tenecteplase for stroke at 4.5 to 24 hours with perfusion-imaging selection (TIMELESS). N Engl J Med. 2024;390(8):701-11. doi: 10.1056/NEJMoa2310392.
Roaldsen MB, Eltoft A, Wilsgaard T, Christensen H, Engelter ST, Indredavik B, et al. Safety and efficacy of tenecteplase in patients with wake-up stroke assessed by non-contrast CT (TWIST): a multicentre, open-label, randomised controlled trial. Lancet Neurol. 2023;22(2):117-26. doi: 10.1016/S1474-4422(22)00484-7.
Xiong Y, Campbell BCV, Fisher M, Schwamm LH, Parsons M, Li H, et al. Rationale and design of tenecteplase reperfusion therapy in acute ischaemic cerebrovascular events III (TRACE III): a randomised, phase III, open-label, controlled trial. Stroke Vasc Neurol. 2024;9(1):82-9. doi: 10.1136/svn-2023-002310.
Bivard A, Zhao H, Churilov L, Campbell BCV, Coote S, Yassi N, et al. Comparison of tenecteplase with alteplase for the early treatment of ischaemic stroke in the Melbourne Mobile Stroke Unit (TASTE-A): a phase 2, randomised, open-label trial. Lancet Neurol. 2022;21(6):520-7. doi: 10.1016/S1474-4422(22)00171-5.
Gao L, Parsons M, Churilov L, Zhao H, Campbell BCV, Yan Bernard, et al. Cost-effectiveness of tenecteplase versus alteplase for stroke thrombolysis evaluation trial in the ambulance. Eur Stroke J. 2023;8(2):448-55. doi:10.1177/23969873231165086.
Luo Z, Zhou Y, He Y, Yan S, Chen Z, Zhang X, et al. Treatment with intravenous alteplase in ischaemic stroke patients with onset time between 4.5 and 24 hours (HOPE): protocol for a randomised, controlled, multicentre study. Stroke Vasc Neurol. 2024;9(3):318-23. doI: 10.1136/svn-2022-002154.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2025 สมาคมเภสัชกรรมโรงพยาบาล(ประเทศไทย)

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมโรงพยาบาลทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสาร (สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย)) อย่างเป็นลายลักษณ์อักษร
สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) อนุญาตให้สามารถนำไฟล์บทความไปใช้ประโยชน์และเผยแพร่ต่อได้ โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอน (Creative Commons License: CC) โดย ต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง, Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ


