
The Efficacy of Using Sedation Protocol on Medication Error of Proportion Drug Use and Incidence Rate of Unplanned Extubation in Intensive Care Unit
Keywords:
medication error, unplanned extubation, sedation protocolAbstract
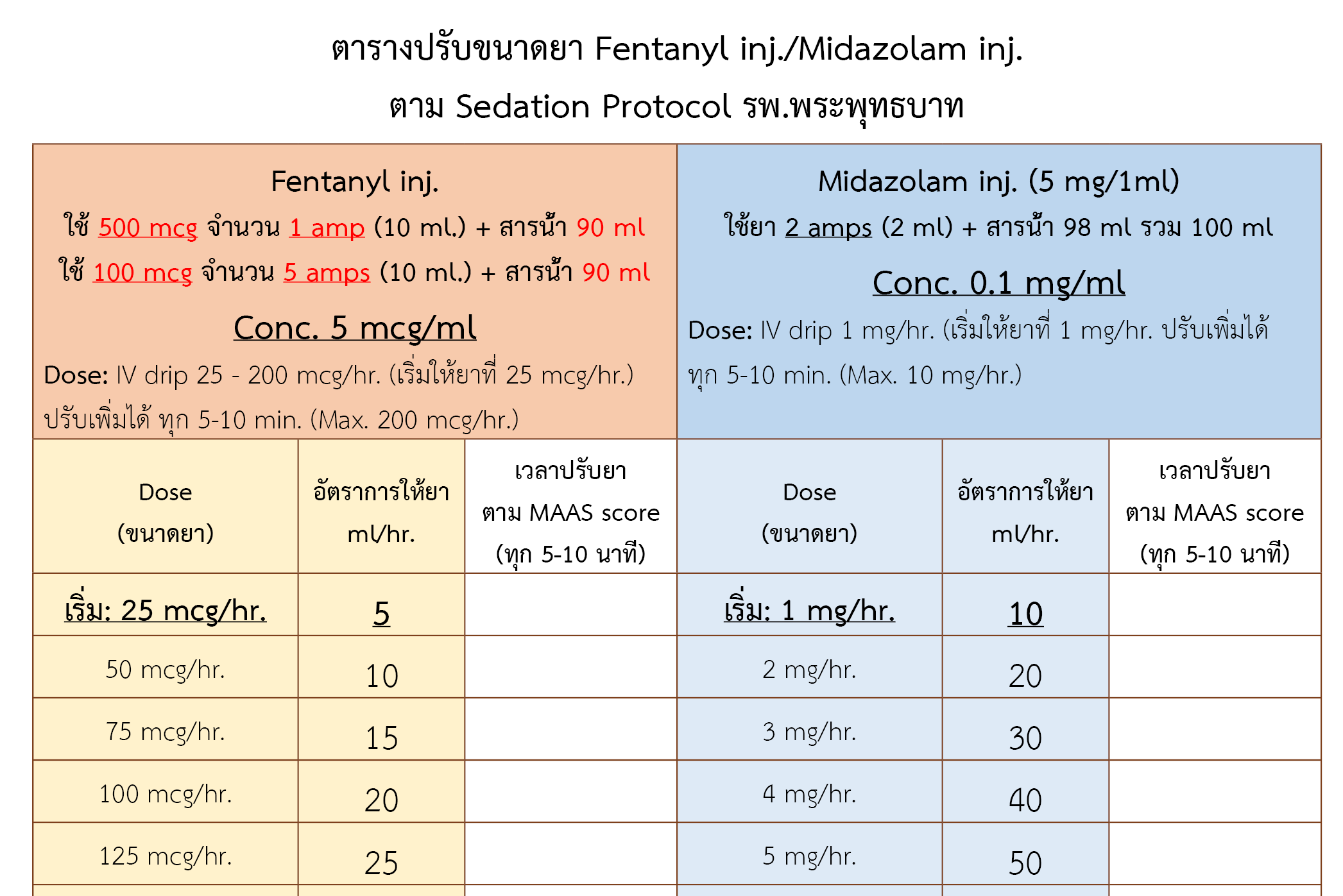
Background: Prescribing errors and administration errors occurred with proportion use of fentanyl and midazolam injection for endotracheal intubated patients. Nurses caring of these patients experienced problems to interpret medication orders because there are no clear guidelines. It was found that these 2 drugs were mostly used in intensive care unit (ICU). It was also found that the incidence rate of unplanned extubation (UE) was higher than the target. Therefore, a sedation protocol has been developed. It is expected that these problems can be solved.
Objectives: The purpose of this study was to examine the effect of sedation protocol on medication error, UE rate, and determine physicians and nurses satisfaction of this sedation protocol.
Method: This is quasi-experimental study. Data of patients in ICU between November 15, 2022 - February 15, 2023 were collected. The results were analyzed using descriptive statistics, Fisher’s exact test and Chi-squared test.
Results: After the sedation protocol was implemented, prescribing error and administration error were significantly decreased from 2.68% (9/336) to 0% (0/527) (p-value < 0.001). The incidence rate of UE in ICU was significantly decreased from 13.19% (15.67 episodes per 1,000 device days) to 2.70% (2.43 episodes per 1,000 device days) (p-value < 0.016). There were 96% of physicians and nurses (n=50) who satisfied at level of ≥4 satisfaction scores with the use of the sedation protocol (mean=4.34/5, standard deviation=0.56).
Conclusion: The use of sedation protocol can help prevent medication errors of proportion drug use and reduce the incidence rate of UE in ICU. Physicians and nurses satisfied with the use of the sedation protocol.
References
Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. 2014; 370(5):444-54. doi: 10.1056/NEJMra1208705.
Stein-Parbury J, McKinley S. Patients’experiences of being in an intensive care unit: a select literature review. Am J Crit Care. 2000;9(1):20-7. PMID: 10631387.
Barr J, Fraser GL, Puntillo K, Puntillo K, Ely EW, Gélinas C, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263-306. doi: 10.1097/CCM.0b013e3182783b72.
Fraser GL, Prato BS, Riker RR, Berthiaume D, Wilkins ML. Frequency, severity, and treatment of agitation in young versus elderly patients in the ICU. Pharmacotherapy. 2000;20(1):75-82. doi: 10.1592/phco.20.1.75.34663.
da Silva PS, Fonseca MC. Unplanned endotracheal extubations in the intensive care unit: systematic review, critical appraisal, and evidence-based recommendations. Anesth. Analg. 2012;114(5):1003-14. doi: 10.1213/ANE.0b013e31824b0296.
สมจิตต์ แสงศรี. การพัฒนาและประเมินผลแนวปฏิบัติการพยาบาลเพื่อป้องกันการถอดท่อช่วยหายใจโดยไม่ได้วางแผนในหออภิบาลผู้ป่วยศัลยกรรม โรงพยาบาลสงขลานครินทร์ [วิทยานิพนธ์ปริญญาพยาบาลศาสตรมหาบัณฑิต (การพยาบาลผู้ใหญ่)]. สงขลา: มหาวิทยาลัยสงขลานครินทร์; 2555.
Patel SB, Kress JP. Sedation and analgesia in the mechanically ventilated patient. Am J Respir Crit Care Med. 2012;185(5):486-97. doi: 10.1164/rccm.201102-0273CI.
Huang YT. Factors leading to self-extubation of endotracheal tubes in the intensive care unit. Nurs Crit Care. 2009;14(2):68-74. doi: 10.1111/j.1478-5153.2008.00320.x.
มังกร ประพันธ์วัฒนะ. การจัดการยาที่ต้องระมัดระวังสูง. ใน: มังกร ประพันธ์วัฒนะ, บรรณาธิการ. ระบบยาเพื่อความปลอดภัย. กรุงเทพฯ: สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย); 2553. หน้า 259-86.
ฐิติมา ด้วงเงิน, ชานนท์ หนูสวัสดิ์, ศุภาพิชญ์ สกุลเวช. ความเข้าใจคำสั่งใช้ยาแบบอัตราส่วนในกลุ่มยาที่มีความเสี่ยงสูงของพยาบาลวิชาชีพและการคำนวณเพื่อเตรียมยาตามคำสั่งใช้ยา. วารสารเภสัชกรรมไทย [อินเทอร์เน็ต]. 2559 [สืบค้นเมื่อ 17 ก.ค. 2566];8(1):128-38. สืบค้นจาก: https://he01.tci-thaijo.org/index.php/TJPP/article/view/169707
อภิฤดี เหมะจุฑา. ความปลอดภัยในการใช้ยาที่มีความเสี่ยงสูง [อินเทอร์เน็ต]. นนทบุรี: ศูนย์การศึกษาต่อเนื่องทางเภสัชศาสตร์ สภาเภสัชกรรม; 2560 [สืบค้นเมื่อ 17 ก.ค. 2566]. สืบค้นจาก: https://ccpe.pharmacycouncil.org/index.php?option=article_detail&subpage=article_detail&id=275
สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย). กรอบงานพื้นฐานระบบยา. กรุงเทพฯ: สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย); 2563.
Laselle TJ, May SK. Medication orders are written clearly and transcribed accurately - implementing medication management standard 3.20 and national patient safety goal 2b. Hosp Pharm. 2010;41(1):82-7. doi: 10.1310/hpj4101-82.
ณัฐนิชา กลับสุวรรณ์. ความคลาดเคลื่อนทางยาและการแก้ไขปัญหาของการใช้ยาเคมีบำบัดในผู้ป่วยใน โรงพยาบาลอุตรดิตถ์ [วิทยานิพนธ์ปริญญาเภสัชศาสตรมหาบัณฑิต]. เชียงใหม่:คณะเภสัชศาสตร์มหาวิทยาลัยเชียงใหม่; 2549.
ฉัตรสุดา จำรัส, ขนิษฐา แก้วพรม, สายพิณ โสภารัตนากูล, เทวัญ ยอดยิ่ง, นราวิชญ์ เหล่ากาวี. ประสิทธิผลของการใช้แนวปฏิบัติทางคลินิกสำหรับการป้องกันความคลาดเคลื่อนในการบริหารยาแก่ผู้ป่วย โรงพยาบาลแพร่. วารสารโรงพยาบาลแพร่ [อินเทอร์เน็ต]. 2565 [สืบค้นเมื่อ 17 ก.ค. 2566];30(2):43-55. สืบค้นจาก: https://thaidj.org/index.php/jpph/article/view/12848/10812
มณีนุช สุทธสนธิ์, ขนิษฐา แก้วกัลยา, วาสนา นัยพัฒน์. ผลของการใช้แนวปฏิบัติการพยาบาลต่ออัตราการเกิดท่อช่วยหายใจเลื่อนหลุดในผู้ป่วยอาการหนักที่ใส่ท่อช่วยหายใจ. วารสารการพยาบาลและการศึกษา [อินเทอร์เน็ต]. 2560 [สืบค้นเมื่อ 17 ก.ค. 2566];10(2):58-70. สืบค้นจาก: https://he01.tci-thaijo.org/index.php/JNAE/article/view/122507
สมพร นรขุน, รัชนี นามจันทรา, วารินทร์ บินโฮเซ็น. ผลของการใช้แนวปฏิบัติการพยาบาลต่ออัตราการเกิดการถอดท่อช่วยหายใจโดยไม่ได้วางแผนในผู้ป่วยใส่ท่อช่วยหายใจ. วารสารพยาบาลโรคหัวใจและทรวงอก [อินเทอร์เน็ต]. 2559 [สืบค้นเมื่อ 17 ก.ค. 2566];27(1):72-84. สืบค้นจาก: https://he02.tci-thaijo.org/index.php/journalthaicvtnurse/article/view/69766
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2023 Association of Hospital Pharmacy (Thailand)

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมโรงพยาบาลทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสาร (สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย)) อย่างเป็นลายลักษณ์อักษร
สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) อนุญาตให้สามารถนำไฟล์บทความไปใช้ประโยชน์และเผยแพร่ต่อได้ โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอน (Creative Commons License: CC) โดย ต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง, Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับสมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย) และบุคลากรในสมาคมฯ แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ


