ช่วงค่าอ้างอิงฮอร์โมนไทรอยด์สติมูเลติงของทารกเกิดก่อนกำหนดและน้ำหนักแรกเกิดน้อย
ช่วงค่าอ้างอิงฮอร์โมนไทรอยด์สติมูเลติงของทารก
คำสำคัญ:
ฮอร์โมนไทรอยด์สติมูเลติง, ช่วงค่าอ้างอิง, เกิดก่อนกำหนด, ทารกน้eหนักแรกเกิดน้อย, ภาวะพร่องฮอร์โมนไทรอยด์แต่กำเนิดบทคัดย่อ
ทารกเกิดก่อนกำหนดและ/หรือทารกน้ำหนักแรกเกิดน้อย มีระดับ thyroid stimulating hormone (TSH) ต่ำ ทำให้การตรวจคัดกรองได้ผลลบลวงและไม่พบทารกที่เป็นภาวะพร่องฮอร์โมนไทรอยด์แต่กำเนิด (congenital hypothyroidism) เพื่อหาช่วงค่าอ้างอิง (reference intervals; RIs) ที่ 2.5th-97.5th percentile และเวลาที่เหมาะสมสำหรับตรวจคัดกรองซ้ำ การศึกษานี้ได้วิเคราะห์ระดับ TSH ของทารกแรกเกิดอายุุ 2-7 วัน จากข้อมูลระดับ TSH รวมถึงอายุครรภ์
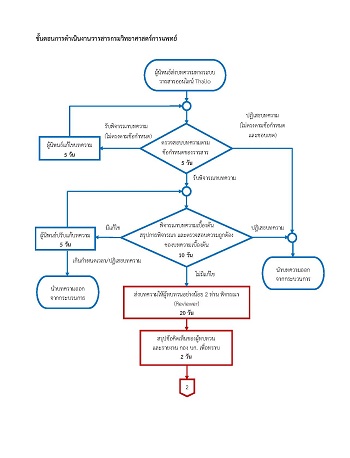
(gestation ages; GAs) หน่วยเป็นสัปดาห์ และน้ำหนักแรกเกิด (birth weights; BWs) หน่วยเป็นกรัม ย้อนหลัง 2 ปี (2563–2564) ของศูนย์ปฏิบัติการตรวจคัดกรองสุุขภาพทารกแรกเกิดแห่งชาติ กรมวิทยาศาสตร์การแพทย์ โดยแบ่งทารกเป็น 8 กลุ่ม ตาม GAs และ BWs พบว่า BW ที่ต่ำลงไม่มีผลต่อระดับ TSH ของทารกเกิดที่ GA ≥ 37 ในขณะที่ ระดับ TSH ของทารกเกิดที่ GA ≤ 36 มีแนวโน้มต่ำลงตาม GA และ BW ที่ลดลงของทารก ผลการศึกษาพบว่าระดับ TSH ของทารกเกิดที่่ GA 32-36 มีค่าใกล้เคียงกับทารกเกิดครบกำหนด โดยกลุ่ม ทารกที่มี BW มากกว่าหรือเท่ากับ 2,500, 1,500–2,499 และ 1,000–1,499 มี TSH RIs (ในหน่วย mU/L) เท่ากับ 1.67–13.68, 1.56–13.81 และ 0.93–14.46 ตามลำดับ ในขณะที่ทารกเกิดที่ GA < 32 มีค่า TSH RIs ต่ำลงอย่างเห็นได้ชัดในช่วง 0.07–7.22, 0.89–10.14 และ 1.14–10.67 สำหรับทารกเกิดที่ GA < 28 BW < 1,000–2,499, GA 28–31 BW 1,000–1,499 และ GA 28–31 BW 1,500–2,499 ตามลำดับ ดังนั้นเพื่อป้องกันการเกิดผลลบลวงจากการตรวจคัดกรอง TSH ในทารกเกิดก่อนกำหนด จึงควรตรวจซ้ำที่อายุของทารกนับจากวันที่มารดามีประจำเดือนครั้งสุุดท้ายจนถึงปัจจุบันที่ 32 สัปดาห์ และ ≥ 34 สัปดาห์ ตามลำดับ
เอกสารอ้างอิง
Charoensiriwatana W, Janejai N, Boonwanich W, Krasao P, Chaisomchit S, Waiyasilp S. Neonatal screening program in Thailand. Southeast Asian J Trop Med Public Health 2003; 34(Suppl 3): 94-100.
Atteih S, Ratner J, Endocrinology. In: Klein K, Mcdaniel L, Molloy M, editors. The harriet lane book. 22nd ed. Philadelphia: Elsevier; 2021. p. 235-239.
Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis 2010; 5: 17. (22 pages).
Yarahmadi SH, Tabibi SJ, Alimohammadzadeh Kh, Ainy E, Gooya MM, Mojarrad M, et al. Cost-benefit and effectiveness of newborn screening of congenital hypothyroidism: Findings from a national program in Iran. Int J Endocrinol Metab 2010; 1: 1-6.
สมาคมต่อมไร้ท่อเด็กและวัยรุ่นไทย. แนวทางการวินิจฉัยและรักษา Congenital Hypothyroidism. [ออนไลน์]. กุมภาพันธ์ 2564; [สืบค้น 6 พ.ค. 2564]; [9 หน้า]. เข้าถึงได้ที่: URL: https://thaipedendo.org/guideline-for-congenital-hypothyroidism/.
Nagasaki K, Minamitani K, Anzo M, Adachi M, Ishii T, Onigata K, et al.Guidelines for mass screening of congenital hypothyroidism (2014 revision). Clin Pediatr Endocrinol 2015; 24(3): 107-33.
Büyükgebiz A. Newborn screening for congenital hypothyroidism. J Clin Res Pediatr Endocrinol 2013; 5(Suppl 1): 8-12.
เปี่ยมนุกูล กระเสาร์, เพ็ญพรรณ ทองเงา, จารณี พึ่งโพธิ์สภ, วิยะดา เจริญศิริวัฒน์, หรรษา ไทยศรี, อาชวินทร์ โรจนวิวัฒน์. ภาวะพร่องไทรอยด์ฮอร์โมนแต่กำเนิดในทารกแรกเกิดใน 4 ภูมิภาคของประเทศไทยช่วงปี พ.ศ. 2559 ถึง 2561. ว กรมวิทย พ 2564; 63(2): 259-74.
Niwa F, Kawai M, Kanazawa H, Iwanaga K, Matsukura T, Hasegawa T, et al. Hyperthyrotropinemia at 2 weeks of age indicates thyroid dysfunction and predicts the occurrence of delayed elevation of thyrotropin in very low birth weight infants. Clin Endocrinol 2012; 77(2): 255-61.
Léger J, Olivieri A, Donaldson M, Torresani T, Krude H, Vliet GV, et al. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. J Clin Endocrinol Metab 2014; 99(2): 363-84.
Jayasuriya MS, Choy KW, Chin LK, Doery J, Stewart A, Bergman P, et al. Reference intervals for neonatal thyroid function tests in the first 7 days of life. J Pediatr Endocrinol Metab. 2018; 31(10): 1113-6.
LaFranchi SH. Thyroid function in preterm/low birth weight infants: impact on diagnosis and management of thyroid dysfunction. Front Endocrinol. 2021; 12: 666207. (9 pages).
Clark SJ, Deming DD, Emery JR, Adams LM, Carlton EI, Nelson JC. Reference ranges for thyroid function tests in premature infants beyond the first week of life. J Perinatol 2001; 21(8): 531-6.
Kaluarachchi DC, Allen DB, Eickhoff JC, Dawe SJ, Baker MW. Thyroid-stimulating hormone reference ranges for preterm infants. Pediatrics 2019; 144(2): e20190290. (7 pages).
Wang Y, Wu X, Hong K, Fu X, Chen T, Zhu M, et al. Establishment of reference intervals for thyroid hormones in premature infants beyond the first week of life using Beckman Coulter Unicel DxI 800. Clin Biochem 2019; 74: 19-23.
World Health Organization. Preterm birth. [online]. 2018; [cited 2022 Jan 16]; [131 screens]. Available from: URL: https://www.who.int/news-room/fact-sheets/detail/preterm-birth.
World Health Organization. ICD-10: international statistical classification of diseases and related health problems: tenth revision, 2nd ed. [online]. 2004; [cited 2022 Jan 16]; [131 screens]. Available from: URL: https://apps.who.int/iris/handle/10665/42980.
Magnusson B, Ornemark U, editors. Eurachem guide: the fitness for purpose of analytical method-A laboratory guide to method validation and related topics. 2nd ed. [online]. 2014; [cited 2022 Dec 16]; [62 screens]. Available from: URL: https://www.eurachem.org/index.php/publications/guides/mv.
Westgard JO. Basic method validation. 3rd ed. Madison: Westgard Quality Corporation, Inc; 2008. p. 1-256.
Tukey JW. Exploratory data analysis, volume 2. Addison-Wesley series in behavioral science. Reading, MA: Addison-Wesley Publishing Company; 1977.
Higgins V, Asgari S, Adeli K. Choosing thebest statistical method for reference interval estimation. Clin Biochem 2019; 71: 14-6.
Lafranchi S. Thyroid function in the preterm infant. Thyroid 1999; 9(1): 71-8.
Murphy N, Hume R, Toor HV, Matthews TG, Ogston SA, Wu SY, et al. The hypothalamicpituitary-thyroid axis in preterm infants; changes in the first 24 hours of postnatal life. J Clin Endocrinol Metab 2004; 89(6): 2824-31.
Cavarzere P, Camilot M, Popa FI, Lauriola S, Teofoli F, Gaudino R, et al. Congenital hypothyroidism with delayed TSH elevation in low-birth-weight infants: incidence, diagnosis and management. Eur J Endocrinol 2016; 175: 395-402.
Segura SA, Casano-Sancho P, Guindulain MC. Assessment of thyroid function in the preterm and/or very low birth weight newborn. An Pediatr 2021; 95: 277.e1-8.
Mcgrath N, Hawkes CP, Mayne P, Murphy NP. Optimal timing of repeat newborn screening for congenital hypothyroidism in preterm infants to detect delayed thyroid-stimulating hormone elevation. J Pediatr 2019; 205: 77-82.
Kaluarachchi DC, Allen DB, Eickhoff JC, Dawe SJ, Baker MW. Increased congenital hypothyroidism detection in preterm infants with serial newborn screening. J Pediatr 2019; 207: 220-5.
Jiang X, Huang Y, Feng Y, Tang F, Jia X, Chen Q, et al. Same-sex twin have a high incidence of congenital hypothyroidism and a high probability to be missed at newborn screening. Clin Chim Acta 2020; 502: 111-5.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 วารสารกรมวิทยาศาสตร์การแพทย์

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.