
Pure Flat Epithelial Atypia of the Breast on Core Needle Biopsy: No Need for Surgical Excision
Keywords:
Breast cancer, flat epithelial atypia (FEA), upgrade rateAbstract
Objective: From previous data, pure flat epithelial atypia (FEA) of the breast demonstrated on core needle biopsy (CNB) was related to malignant upgrading. However, FEA itself is not an independent factor for developing breast cancer; therefore, the necessity of subsequent surgical excision is controversial. This study aimed to evaluate the upgrade rate of FEA after surgical excision and to demonstrate the necessity of surgical excision in FEA lesions identified on CNB.
Materials and Methods: This retrospective study involved a review of the clinical features, mammographic and ultrasound findings, and pathological reports of patients with pure FEA found from CNB specimens between January 2010 to January 2019. FEA accompanied with atypical ductal hyperplasia, atypical lobular hyperplasia, ductal carcinoma in situ (DCIS), and invasive cancer (IC) in ipsilateral breast were excluded. FEA upgrade is defined as patients with in situ or invasive cancer presented in surgical excision specimens. The breast imaging results of pure FEA and FEA upgrade subsets were compared.
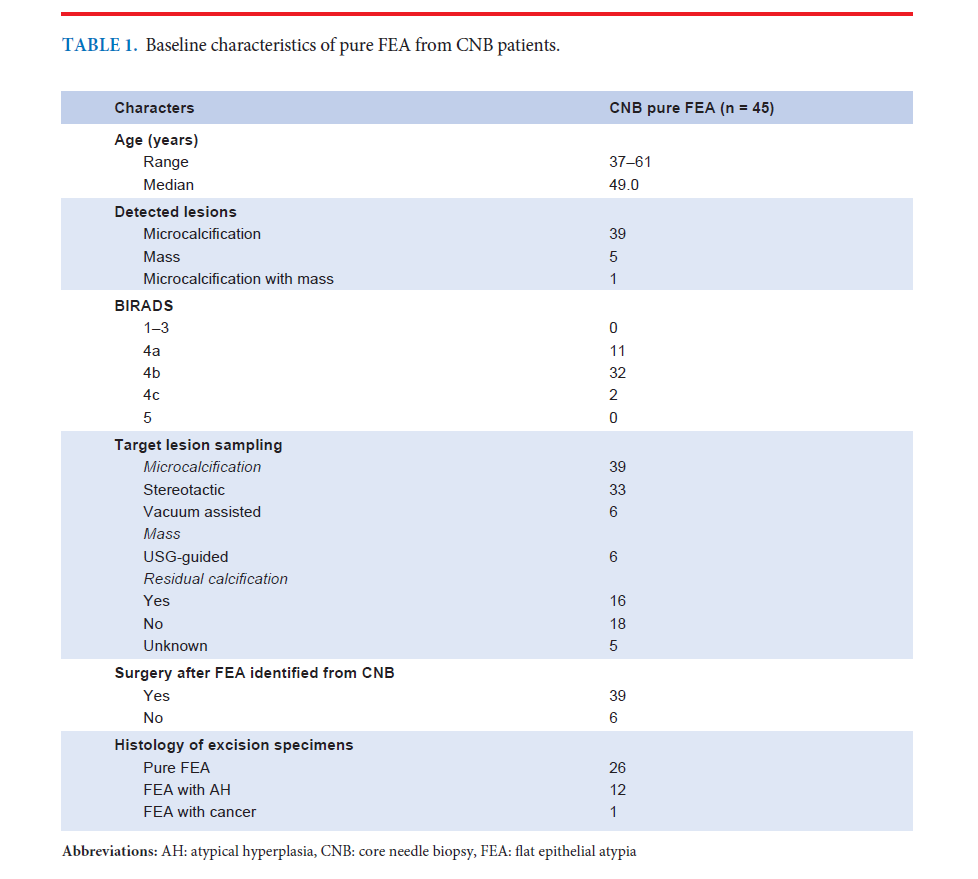
Results: In total, 45 pure FEA specimens were revealed from CNB; of which, 6 of the pure FEA (13.33%) did not undergo further surgical excision, however, they showed no recurrence during follow-up (median follow-up time: 2.68 years). The majority of FEA cases were detected by mammography in 39 patients (86.67%). Of the 45 patients, 32 were classified into BI-RADS 4B (71.11%), 11 as BI-RADS 4A (24.44%), and 2 as BI-RADS 4C (4.44%). One patient was upgraded to DCIS (2.7%). BI-RADS classification did not differ between upgrade FEA and non-upgrade FEA groups (p=0.49).
Conclusion: Only a 2.7% upgrade rate, omitting the surgical excision of pure FEA from CNB, was possible. Even though our study could not demonstrate a correlation between FEA upgrade and radiological findings, BIRADS 4A was less likely to carry the malignant cells. Furthermore, segmental microcalcification tended to be associated with upgraded lesions, but not significantly.
Published
How to Cite
Issue
Section
License
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.





