
Relapse Rate and Clinical Risk Factors Affecting the Treatment of Graves’ Disease
DOI:
https://doi.org/10.33192/Smj.2021.59Keywords:
Relapse; Graves’ disease, antithyroid drugs, risk factorsAbstract
Objective: To determine the relapse rate of Graves’ disease (GD) and identify important clinical risk factors for relapse.
Materials and Methods: This was a 10-year retrospective cohort study. Information was collected with ICD10 E050 codes for Graves’ hyperthyroidism among Thai patients of both sexes and all ages with no history of pregnancy, thyroid storm or antithyroid drug (ATD) allergy.
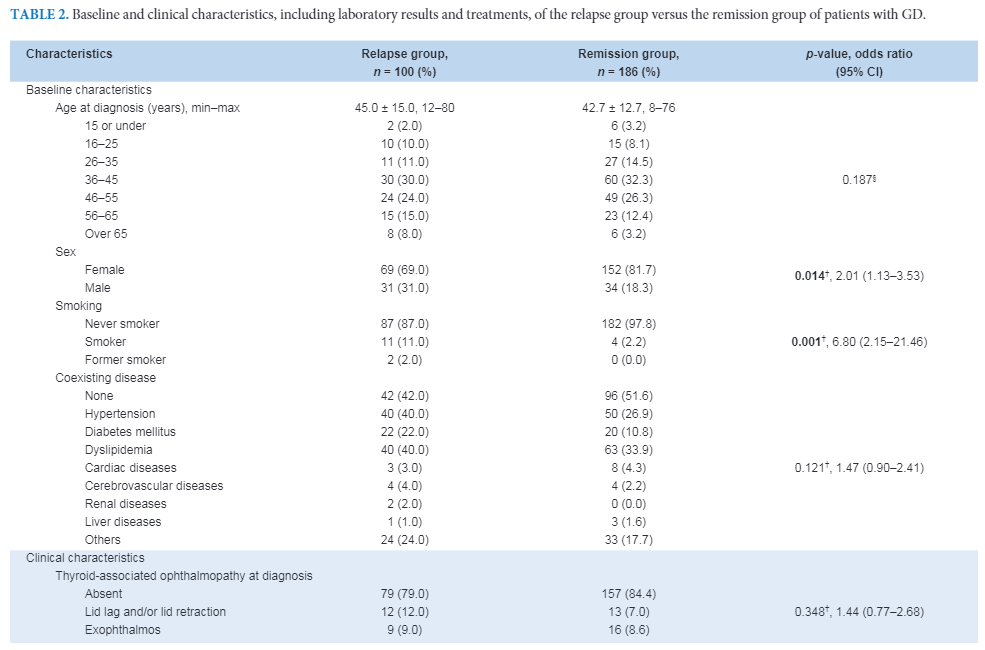
Results: The 286 included GD patients had a relapse rate of 35% after ATD withdrawal for one year. The clinical risk factors associated with relapse were male sex (p = 0.014), smoking (p = 0.001), serum free T4 (FT4) levels > 2 times the upper normal range at diagnosis (p = 0.005), duration for maintenance treatment < 6 and 9 months (p < 0.005) compared with remission. A TSH level < 1 mIU/L (p = 0.060) and MMI > 2.5 mg per day before ATD withdrawal (p = 0.094) trended toward associations with relapse. The clinical factors that predicted GD relapse were serum FT4 levels at diagnosis (p = 0.006) and serum free T3 (FT3) levels before ATD withdrawal (p = 0.019).
Conclusion: Male sex, smoking and serum FT4 levels at diagnosis > 2 times the normal range were significant clinical factors for GD relapse in Thai patients. To reduce the relapse rate in the first year, MMI should be used in maintenance periods for 9 to 12 months with serum FT3 levels within low-normal ranges before ATD withdrawal. This would promote future guidelines for GD management in Thailand.
References
2. Burch HB, Burman KD, Cooper DS. A 2011 survey of clinical practice patterns in the management of Graves’ disease. J Clin Endocrinol Metab 2012;97:4549-58.
3. Sriphrapradang C. Diagnosis and management of Graves’ disease in Thailand: A Survey of current practice. Journal of Thyroid Research, vol.2020, Article ID 8175712, 8 pages.
4. Bartalena L, Burch HB, Burman KD, Kahaly GJ. A 2013 European survey of clinical practice patterns in the management of Graves’ disease. Clin Endocrinol (Oxf) 2016;84:115-20.
5. Burch HB, Cooper DS. Antithyroid drugs therapy: 70 years later. Eur J Endocrinol 2018;179:R261-74.
6. Kahaly GJ, Bartalena L, Hegedus L, Leenhardt L, Poppe K, Pearce SH. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. Eur Thyroid J 2018;7:167-86.
7. Laurberg P. Remission of Graves' disease during anti-thyroid drug therapy. Time to reconsider the mechanism? Eur J Endocrinol 2006;155:783-6.
8. Klein I, Becker DV, Levey GS. Treatment of hyperthyroid disease. Ann Intern Med 1994;121:281-8.
9. Mazza E, Carlini M, Flecchia D, Blatto A, Zuccarini O, Gamba S, et al. Long-term follow-up of patients with hyperthyroidism due to Graves' disease treated with methimazole. Comparison of usual treatment schedule with drug discontinuation vs continuous treatment with low methimazole doses: a retrospective study. J Endocrinol Invest 2008;31:866-72.
10. Mohlin E, Filipsson Nystrom H, Eliasson M. Long-term prognosis after medical treatment of Graves' disease in a northern Swedish population 2000-2010. Eur J Endocrinol 2014;170:419-27.
11. Konishi T, Okamoto Y, Ueda M, Fukuda Y, Harusato I, Tsukamoto Y, et al. Drug discontinuation after treatment with minimum maintenance dose of an antithyroid drug in Graves' disease: a retrospective study on effects of treatment duration with minimum maintenance dose on lasting remission. Endocr J 2011;58:95-100.
12. Liu L, Lu H, Liu Y, Liu C, Xun C. Predicting relapse of Graves' disease following treatment with antithyroid drugs. Exp Ther Med 2016;11:1453-8.
13. Park S, Song E, Oh H-S, Kim M, Jeon MJ, Kim WG, et al. When should antithyroid drug therapy to reduce the relapse rate of hyperthyroidism in Graves’ disease be discontinued? Endocrine 2019;65:348-56.
14. Anagnostics P, Adamidou F, Polyzos SA, Katergari S, Karathanasi E, Zouli C, et al. Predictors of long-term remission in patients with Graves' disease: a single center experience. Endocrine 2013;44:448-53.
15. Lawgaly SA, Kallousa HA, Gerryo S. Predictors of relapse in Graves' hyperthyroidism after treatment with antithyroid drugs. Ibnosina J Med Biomed Sci 2018;10:205-8.
16. Abraham P, Avenell A, Park CM, Watson WA, Bevan JS. A systematic review of drug therapy for Graves' hyperthyroidism. Eur J Endocrinol 2005;153:489-98.
17. Kimball LE, Kulinskaya E, Brown B, Johnston C, Farid NR. Does smoking increase relapse rates in Graves' disease? J Endocrinol Invest 2002;25:152-7.
18. Allahabadia A, Daykin J, Holder RL, Sheppard MC, Gough SC, Franklyn JA. Age and gender predict the outcome of treatment for Graves' hyperthyroidism. J Clin Endocrinol Metab 2000;85:1038-42.
19. Nedrebo BG, Holm PI, Uhlving S, Sorheim JI, Skeie S, Eide GE, et al. Predictors of outcome and comparison of different drug regimens for the prevention of relapse in patients with Graves' disease. Eur J Endocrinol 2002;147:583-9.
20. Orunesu E, Bagnasco M, Salmaso C, Altrinetti V, Bernasconi D, Monte PD, et al. Use of an artificial neural network to predict Graves' disease outcome within 2 years of drug withdrawal. Eur J Clin Invest 2004;34:210-7.
21. Bolaños F, González-Ortiz M, Durón H, Sánchez C. Remission of Graves' hyperthyroidism treated with methimazole. Rev Invest Clin 2002;54:307-10.
22. Harinsoot Somnuke P, Pusuwan P, Likitmaskul S, Santiprabhob S, Sawathiparnich P. Treatment outcome of Graves’ disease in Thai children. J Med Assoc Thai 2007;90:1815-20.
23. Thewjitcharoen Y, Karndumri K, Chatchomchuan W, Porramatikul S, Krittiyawong S, Wanothayaroj E. et al. Serum T3 level and duration of minimum maintenance dose therapy predict relapse in methimazole-treated Graves’ disease. J Endocr Soc 2021;5:1-11.
24. Davies TF LP. Thyrotoxicosis. In: Kronenberg HM, Melmed S, Polonsky KS, Larsen PR. 11th Williams textbook of endocrinology: Philadephia: Saunders, 2008.p.342-55.
25. Vos XG., Endert E., Zwinderman AH., Tijssen JGP., Wiersinga WM. Predicting the risk of recurrence before the start of antithyroid drug therapy in patients with Graves' hyperthyroidism. J Clin Endocrinol Metab 2016;101:1381-9.
26. Park S, Song E, Oh H-S, Kim M, Jeon MJ, Kim WG, et al. When should antithyroid drug therapy to reduce the relapse rate of hyperthyroidism in Graves’ disease be discontinued? Endocrine 2019;65:348-56.
27. Shi M, Sheng R, Hu Y, Jiang L, Wang Z, Cui D. Risk factors for the relapse of Graves’ disease treated with antithyroid drugs: A systematic review and meta-analysis. Clin Ther 2020;42:662-75.e4.
28. Anagnostics P, Adamidou F, Polyzos SA, Katergari S, Karathanasi E, Zouli C, et al. Predictors of long-term remission in patients with Graves' disease: a single center experience. Endocrine 2013;44:448-53.
29. Struja T, Fehlberg H, Kutz A, Guebelin L, Degen C, Mueller B, et al. Can we predict relapse in Graves’disease? Resullts from a systematic review and meta-analysis. Eur J Endocrinol 2017;176:87-97.
30. Lawgaly SA, Kallousa HA, Gerryo S. Predictors of relapse in Graves' hyperthyroidism after treatment with antithyroid drugs. Ibnosina J Med Biomed Sci 2018;10:205-8.
31. Magri F, Zerbini F, Gaiti M, Capelli V, Ragni A, Rotondi M, et al. Gender influences the clinical presentation and long-term outcome of Graves' disease. Endocr Pract 2016;22:1336-42.
32. Zuhur SS, Yildiz I, Altuntas Y, Bayraktaroglu T, Erol S, Sahin S, et al. The effect of gender on response to antithyroid drugs and risk of relapse after discontinuation of the antithyroid drugs in patients with Graves' hyperthyroidism: a multicentre study. Endokrynol Pol 2020;71:207-212.
33. Brix TH, Hansen PS, Kyvik KO, Hegedus L. Cigarette smoking and risk of clinically overt thyroid disease: A population-based twin case-control study. Arch Intern Med 2000;160:661-6.
34. Nyirenda MJ, Taylor PN, Stoddart M, Beckett GJ, Toft AD. Thyroid-stimulating hormone-receptor antibody and thyroid hormone concentrations in smokers vs nonsmokers with Graves' disease treated with carbimazole. JAMA 2009;301:162-4.
35. Bano A, Gan E, Addison C, Narayanan K, Weaver JU, Tsatlidis V, et al. Age may influence the impact of TRAbs on thyroid function and relapse-risk in patients with Graves' disease. J Clin Endocrinol Metab 2019;104:1378-85.
36. Laurberg P. Remission of Graves' disease during anti-thyroid drug therapy. Time to reconsider the mechanism? Eur J Endocrinol 2006;155:783-6.
37. Kahaly GJ, Bartalena L, Hegedus L, Leenhardt L, Poppe K, Pearce SH. 2018 European Thyroid Association guideline for the management of Graves' hyperthyroidism. Eur Thyroid J 2018;7:167-86.
38. Klein I, Becker DV, Levey GS. Treatment of hyperthyroid disease. Ann Intern Med 1994;121:281-8.
39. Abraham P, Avenell A, Watson WA, Park CM, Bevan JS. Antithyroid drug regimen for treating Graves' hyperthyroidism. Cochrane Database Syst Rev 2004 (2);CD003420.
40. Abraham P, Avenell A, Park CM, Watson WA, Bevan JS. A systematic review of drug therapy for Graves' hyperthyroidism. Eur J Endocrinol 2005;153:489-98.
Published
How to Cite
Issue
Section
License
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









