
Intraoperative Problems and Solutions in Pneumovesicum Laparoscopic Cross-trigonal Ureteral Reimplantation in Children by a Beginner Surgeon
DOI:
https://doi.org/10.33192/Smj.2021.98Keywords:
Pneumovesicum LaparoscopicAbstract
Objective: Many beginner surgeons feel anxious when first doing the procedure. Some may encounter many intraoperative difficulties or problems, resulting in abandoning the technique. We will demonstrate our methods and the solutions to major intraoperative problems.
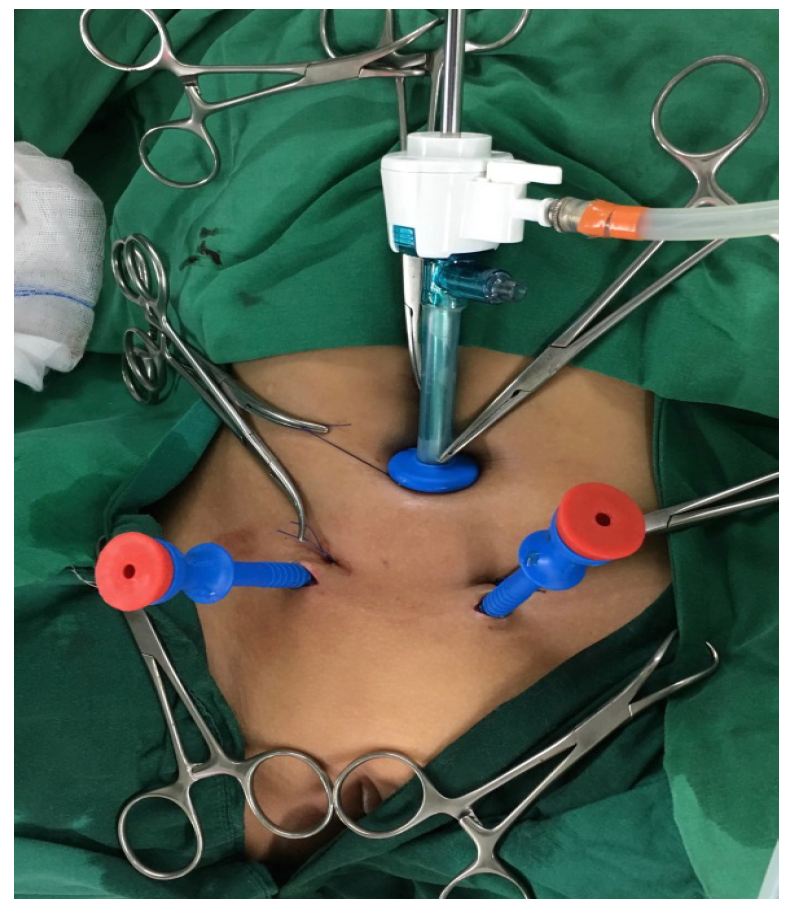
Materials and Methods: A beginner surgeon performed the operation on 13 children with VUR (20 ureters) who met the indications for surgery between October 2016 and August 2017. Age ranged from 2 to 7 years. Each operation comprised 2 main steps: anchoring the urinary bladder wall to the anterior abdominal wall under cystoscopic vision, followed by a cross-trigonal ureteral reimplantation under pneumovesicum laparoscopy. The intraoperative problems, postoperative care, and follow-up periods were recorded to identify surgical outcomes.
Results: Most significant, intraoperative problems were air leakage, bleeding, tear of the bladder mucosa above the tunnel, and inability to insert a tube into the ureter pre- and post-reimplantation. Most problems could be managed. Only one case had to be converted to open reimplantation due to uncontrolled air leakage. Postoperatively, 2 patients had hydroureteronephrosis at 4 weeks, but it eventually spontaneously regressed. One patient had cystitis, treated with oral antibiotics. Between the 1-year and 4-year follow-up, no patients had hydroureteronephrosis or urinary tract infections (UTI).
Conclusion: Pneumovesicum laparoscopic ureteral reimplantation is a feasible technique for beginner surgeons. Although many intraoperative problems may be encountered, most can be managed, resulting in the completion of the laparoscopic procedure.
References
2. Raju GA, Marks AJ, Benoit RM, Docimo SG. Models of care for vesicoureteral reflux with and without an end point of reflux resolution: A computer cost analysis. J Urol. 2013;189(6):2287–92.
3. Esposito C, Escolino M, Lopez M. Surgical Management of Pediatric Vesicoureteral Reflux: A Comparative Study Between Endoscopic, Laparoscopic, and Open Surgery. J Laparoendosc Adv Surg Tech A. 2016;26(7):574–80.3
4. Yeung CK, Sihoe JD, Borzi PA. Endoscopic cross-trigonal ureteral reimplantation under carbon dioxide bladder insufflation: a novel technique. J Endourol 2005;19:295e9.
5. Gill IS, Ponsky LE, Desai M, Kay R, Ross JH. Laparoscopic cross-trigonal Cohen ureteroneocystostomy: novel technique. J Urol. 2001;166(5):1811–4.
6. Valla JS. Transvesicoscopic cohen ureteric reimplantation for vesico-ureteral reflux in children. Pediatr Endourol Tech. 2007;5(6):39–46.
7. Abraham MK, Viswanath N, Bindu S, Kedari P, Ramakrishnan P, Naaz A, et al. A simple and safe technique for trocar positioning in vesicoscopic ureteric reimplantation. Pediatr Surg Int. 2011;27(11):1223–6.
8. Canon SJ, Jayanthi VR, Patel AS. Vesicoscopic Cross-Trigonal Ureteral Reimplantation: A Minimally Invasive Option for Repair of Vesicoureteral Reflux. J Urol. 2007;178(1):269–73.
Published
How to Cite
Issue
Section
License
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









