
Predictive Value of Right Ventricular Pressure Measurement for Residual Pulmonary Stenosis in Tetralogy Repair
DOI:
https://doi.org/10.33192/Smj.2022.28Keywords:
Tetralogy of Fallot repair, right ventricular pressure, residual pulmonary stenosis, intraoperative assessmentAbstract
Objective: The long-term outcome of tetralogy of Fallot repair depends on an adequate relief of right ventricular outflow tract obstruction and preservation of the pulmonary valve function. Since intraoperative transesophageal echocardiography is not routinely performed in small patients, we postulated that the post-bypass right ventricular pressure measured intraoperatively could predict residual pulmonary stenosis when evaluated by transthoracic echocardiography.
Materials and Methods: Of the 187 patients who underwent tetralogy repair between 2012 and 2019 at Siriraj Hospital, Thailand, 95 with right ventricular pressure measurements and pre-discharge echocardiography were included in the study. Their intraoperative parameters, and postoperative outcomes were analyzed. The tolerable pressure cutoff was determined.
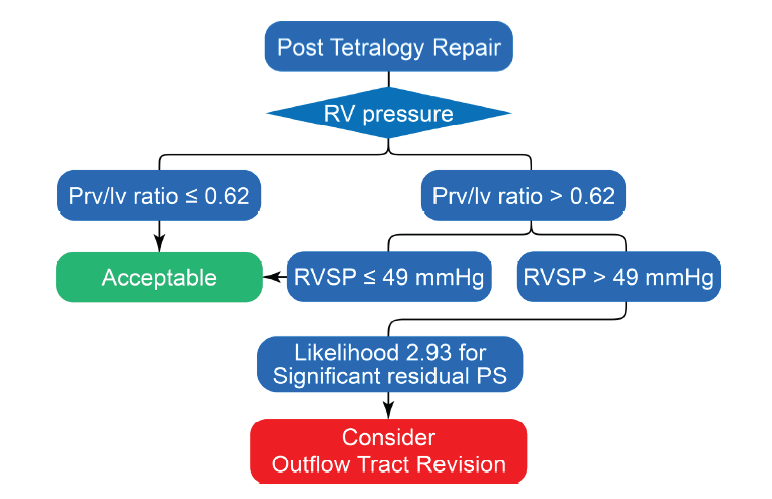
Results: The median patient age was 3.9 years old (interquartile range 2.75–6). Fifty-three patients (54.6%) required the use of the transannular patch. Ten patients (10.3%) had significant residual pulmonary stenosis with a mean right ventricular systolic pressure of 64.0±10.6 mmHg compared with 48.7±14.4 mmHg for the other patients. There was an association between the pressure figure and the degree of residual pulmonary stenosis (rho=0.391, p=0.01). A systolic pressure above 49 mmHg predicted pulmonary stenosis with a likelihood ratio of 2.18 (1.94-2.80, 95%CI). The likelihood rose to 2.93 (2.44-4.01, 95%CI) if the pressure resulted in a right to left ventricular pressure ratio above 0.62. The patients whose figures did not exceed 49 mmHg experienced no significant residual obstruction, regardless of the pressure ratio.
Conclusion: Intraoperative measurement of the right ventricular pressure can predict residual pulmonary stenosis after tetralogy repair with a reassuring cutoff of 49 mmHg
References
Neill CA, Clark EB. Tetralogy of Fallot. The first 300 years. Tex Heart Inst J 1994;21: 272-9.
Boni L, Garcia E, Galletti L, Perez A, Herrera D, Romos V, et al. Current strategies in tetralogy of Fallot repair: pulmonary valve sparing and evolution of right ventricle/left ventricle pressures ratio. Eur J Cardiothorac Surg 2009;35:885-9; discussion 889-890. DOI: 10.1016/j.ejcts.2009.01.016.
Borodinova O, Mykychak Y, Yemets I. Transesophageal Echocardiographic Predictor of Significant Right Ventricular Outflow Tract Obstruction After Tetralogy of Fallot Repair. Semin Thorac Cardiovasc Surg 2020;32:282-9. DOI: 10.1053/j.semtcvs.2019.09.011.
Ferraz Cavalcanti PE, Sa MP, Santos CA, Esmeraldo IM, de Escobar R, de Menezes AM, et al. Pulmonary valve replacement after operative repair of tetralogy of Fallot: meta-analysis and meta-regression of 3,118 patients from 48 studies. J Am Coll Cardiol 2013;62:2227-43. DOI: 10.1016/j.jacc.2013.04.107.
Geva T. Indications and timing of pulmonary valve replacement after tetralogy of Fallot repair. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2006;11-22. DOI: 10.1053/j.pcsu.2006.02.009.
Egbe AC, Vallabhajosyula S, Connolly HM. Trends and outcomes of pulmonary valve replacement in tetralogy of Fallot. Int J Cardiol 2020;299:136-9. DOI: 10.1016/j.ijcard.2019.07.063.
Gellis L, Banka P, Marshall A, Emani S, Porras D. Transcatheter balloon dilation for recurrent right ventricular outflow tract obstruction following valve-sparing repair of tetralogy of Fallot. Catheter Cardiovasc Interv 2015;86:692-700. DOI:10.1002/ccd.25930.
Chittithavorn V, Rergkliang C, Chetpaophan A, Vasinanukorn P, Sopontammarak S, Promphan W. Predicted outcome after repair of tetralogy of Fallot by postoperative pressure ratio between right and left ventricle. J Med Assoc Thai 2006;89:43-50.
Naito Y, Fujita T, Manabe H, Kawashima Y. The criteria for reconstruction of right ventricular outflow tract in total correction of tetralogy of Fallot. J Thorac Cardiovasc Surg 1980;80:574-81.
Kaushal SK, Radhakrishanan S, Dagar KS, Lyer PU, Girotra S, Shrivastava S, et al. Significant intraoperative right ventricular outflow gradients after repair for tetralogy of Fallot: to revise or not to revise? Ann Thorac Surg 1999;68:1705-12; discussion 1712-3. DOI: 10.1016/s0003-4975(99)01069-3.
Published
How to Cite
Issue
Section
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









