
Early Surgical Complications Following Transanal Endorectal Pull-through for Hirschsprung’s Disease
DOI:
https://doi.org/10.33192/smj.v75i6.261710Keywords:
Hirschsprung, endorectal pullthrough, complications, anastomosis, bowel preparationAbstract
Objective: The purpose of this study was to examine factors affecting early complications following transanal endorectal pull-through (TERPT) in patients with Hirschprung’s disease.
Materials and Methods: Retrospective chart reviews of patients with Hirschsprung’s disease who underwent TERPT/ abdominal assisted TERPT at Siriraj Hospital between January 2009 and December 2019 was carried out. .
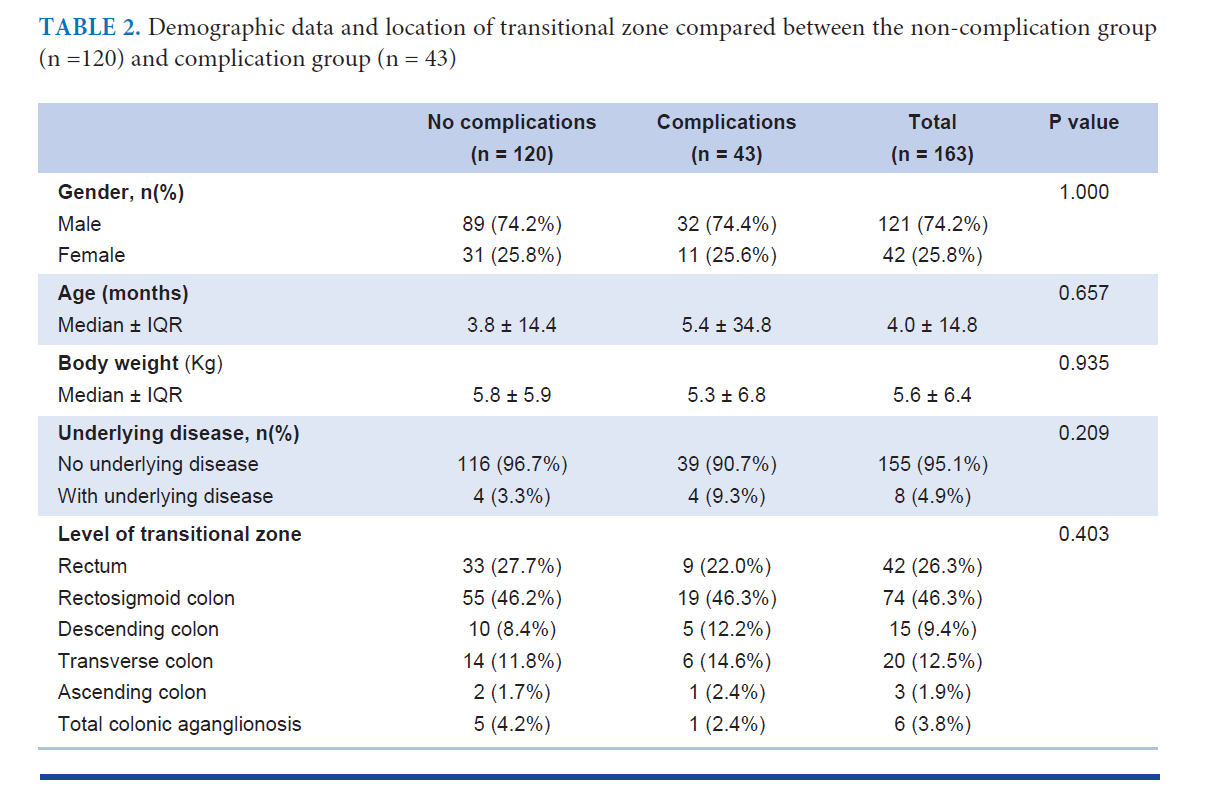
Results: The overall complication rate was 26% (43/163). The complications were as follows: 14 cases of anastomotic strictures (32.6%), five cases of abscess at anastomosis (11.6%), and three cases of anastomotic leakages (7.0%). In regards to preoperative bowel preparation, when comparing those with and those without post-operative complications, the amount of NSS for rectal irrigation (ml/Kg), duration required (days), and duration of changed diet (days) were the same. Colostomy prior to a pull-through operation could not prevent post-operative complications following endorectal pull-through (p = 1.000). The incidences of early complications following TERPT and abdominal assisted TERPT was the same (p = 0.344). Abdominal assisted TERPT had a higher incidence (4%) of anastomotic leakages whereas TERPT had a higher rate of anastomosis strictures (12%) compared to o abdominal assisted TERPT (5%). The higher the transitional zone, the higher the complication rate. Anastomotic leakages, the most serious complication, rarely occurred following TERPT in the low transitional zone.
Conclusion: There was no significant risk factor associated with early surgical complications following TERPT. Abdominal assisted TERPT should be selected properly according to the level of transitional zone. The complications correlate with whether a perfect pull-through operation could be performed or not.
References
Spouge D, Baird PA. Hirschsprung disease in a large birth cohort. Teratology 1985;32:171-7.
Swenson O. My early experience with Hirschsprung’s disease. J Pediatric Surg 1989;24:839-45.
Soave F. A new surgical technique for the treatment of Hirschsprung’s disease. Surgery 1964;56:1007-14.
Boley SJ. New modification of the surgical treatment of Hirschsprung’s disease. Surgery 1964;56:1015-7.
De la Torre L, Ortega A. Transanal versus open endorectal pull-through for Hirschsprung’s disease. J Pediatr Surg 2000;35:1630-2.
Morowitz MJ, Georgeson KE. Laparoscopic assisted pull-through for Hirschsprung’s disease. In: Holcomb GW, Georgeson KE, Rothenberg SS, eds. In: Atlas of Pediatric Laparoscopy and Thoracoscopy, Philadelphia, Elsevier, 2008.p.101-85.
Teitelbaum DH, Cilley RE, Sherman NJ, Bliss D, Uitvlugt ND, Renaud EJ, et al. A decade of experience with the primary pull-through for Hirschsprung disease in the newborn period: A multicenter analysis of outcomes. Ann Surg 2000; 232:372-80.
So HB, Schwartz DL, Becker JM, Daum F, Schneider KM. Endorectal “pull-through” without preliminary colostomy in neonates with Hirschsprung’s disease. J Pediatr Surg 1980;15:470-1.
Mungnirandr A. Hirschsprung’s disease: Review article. Siriraj Med J 2017:69(4):223-7.
Fortuna RS, Weber TR, Tracy Jr. TF, Silen ML, Cradock TV. Critical analysis of the operative treatment of Hirschsprung’s disease. Arch Surg 1996;131:520-5.
Tariq GM, Brereton RJ, Wright VM. Complications of endorectal pull-through for Hirschsprung’s disease. J Pediatr Surg 1991;26:1202-6.
Little DC, Snyder CL. Early and late complications following operative repair of Hirschsprung’s disease. In: Holschneider AM, Puri P, eds. Hirschsprung’s Disease and Allied Disorders, 3rd ed. New York: Springer; 2008.p.375-85.
Teitelbaum DH, Coran AG. Long-term results and quality of life after treatment of Hirschsprung’s disease and allied disorders. In: Holschneider AM, Puri P, eds. Hirschsprung’s Disease and Allied Disorders, 3rd ed. New York: Springer; 2008.p.389-97.
Hoff N, Wester T, Granström AL. Classification of short-term complications after transanal endorectal pullthrough for Hirschsprung’s disease using the Clavien-Dindo-grading system. Pediatr Surg Int 2019;35(11):1239-43.
Clinical Guidelines (Nursing) ( 2019) . Bowel washout rectal, retrived September,2019, from https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Bowel_washout_rectal/
Colonic irrigation, Children’s Hospital Pittsburgh from http://www.chp.edu/our-services/surgery-pediatric/pediatric-surgery-services-we-offer
Georgeson KE. Hirschsprung’s disease. In: Holcomb III GW, Murphy JA. eds. Ashcraft’s Pediatric Surgery, 5th edition, Philadelphia: Saunders Elsevier; 2010.p.456-67.
Langer JC, Fitzgerald PG, Winthrop AL, Srinathan SK, Foglia RP, Skinner MA, et al. One-stage versus two-stage Soave pull-through for Hirschsprung’s disease in the first year of life. J Pediatr Surg 1996;31:33-7.
Engum SA, Grosfeld JL. Long-term results of treatment of Hirschsprung’s disease. Semin Pediatr Surg 2004;13:273-85.
Nasr A, Langer JC. Evolution of the technique in the transanal pull-through for Hirschsprung’s disease: Effect on outcome. J Pediatr Surg 2007;42:36-40.
Published
How to Cite
License
Copyright (c) 2023 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









