
Human Factors Influencing the Decision to Use Videolaryngoscopes for Intubation in the Operating Room
DOI:
https://doi.org/10.33192/smj.v77i10.275409Keywords:
Videolaryngoscopes, human factors, airway managementAbstract
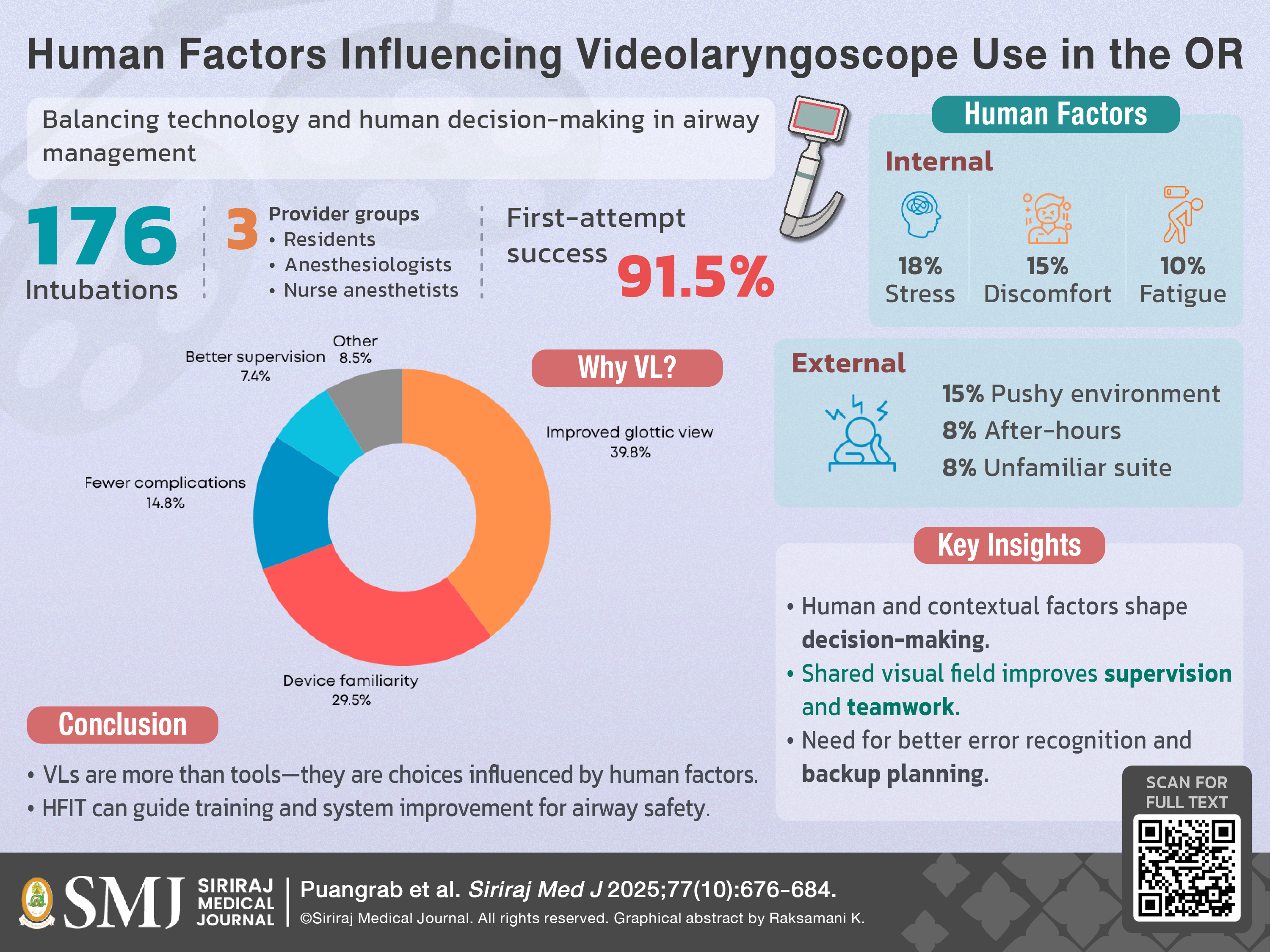
Objective: This study aimed to explore (1) the human factors influencing the decision to use videolaryngoscopes (VLs) instead of conventional Macintosh blades for intubation in operating room settings, and (2) the reasons anesthesia providers report for selecting VLs in clinical practice.
Materials and Methods: A prospective observational study was conducted from September 2020 to June 2021 among anesthesia personnel at Siriraj Hospital. Eligible participants included anesthesiologists, anesthesia residents, and nurse anesthetists who used a VL for intubating adult patients under general anesthesia. Participants completed a structured questionnaire based on the Human Factors Investigation Tool (HFIT) model, which captured internal and external human factors, device selection rationale, and self-assessed performance. Data were analyzed using descriptive and inferential statistics.
Results: A total of 176 VL intubation events were analyzed. Internal human factors such as stress (18.2%), discomfort (15.3%), and fatigue (10.2%), along with external factors like a pushy environment (15.3%) and after-hours work (7.9%), influenced VL use. The most cited reasons for choosing VLs included improved glottic visualization (39.8%), device familiarity (29.5%), fewer complications (14.8%), and better supervision (7.4%). These findings align with key domains of the HFIT model, including situational awareness, decision-making, and environmental conditions.
Conclusion: This study demonstrates that the decision to use VLs is shaped not only by technical considerations but also by a range of human and contextual factors. The HFIT model provided a valuable framework for understanding how providers navigate complex clinical environments. These insights support targeted interventions in training and workplace design to enhance decision-making and airway safety.
References
Lewis SR, Butler AR, Parker J, Cook TM, Schofield-Robinson OJ, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation: a Cochrane Systematic Review. Br J Anaesth. 2017;119(3):369-83.
Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation: a Cochrane systematic review and meta-analysis update. Br J Anaesth. 2022;129(4):612-23.
Ruderman BT, Mali M, Kaji AH, Kilgo R, Watts S, Wells R, et al. Direct vs Video Laryngoscopy for Difficult Airway Patients in the Emergency Department: A National Emergency Airway Registry Study. West J Emerg Med. 2022;23(5):706-15.
Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136(1):31-81.
Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015;115(6):827-48.
Najafi A, Imani F, Makarem J, Khajavi MR, Etezadi F, Habibi S, et al. Postoperative sore throat after laryngoscopy with macintosh or glide scope video laryngoscope blade in normal airway patients. Anesth Pain Med. 2014;4(1):e15136.
Kaplan MB, Hagberg CA, Ward DS, Brambrink A, Chhibber AK, Heidegger T, et al. Comparison of direct and video-assisted views of the larynx during routine intubation. J Clin Anesth. 2006;18(5):357-62.
Schnittker R, Marshall S, Horberry T, Young KL. Human factors enablers and barriers for successful airway management - an in-depth interview study. Anaesthesia. 2018;73(8):980-9.
Kelly FE, Frerk C, Bailey CR, Cook TM, Ferguson K, Flin R, et al. Human factors in anaesthesia: a narrative review. Anaesthesia. 2023;78(4):479-90.
Kelly FE, Frerk C, Bailey CR, Cook TM, Ferguson K, Flin R, et al. Implementing human factors in anaesthesia: guidance for clinicians, departments and hospitals: Guidelines from the Difficult Airway Society and the Association of Anaesthetists: Guidelines from the Difficult Airway Society and the Association of Anaesthetists. Anaesthesia. 2023;78(4):458-78.
Fletcher G, Flin R, McGeorge P, Glavin R, Maran N, Patey R. Anaesthetists' Non-Technical Skills (ANTS): evaluation of a behavioural marker system. Br J Anaesth. 2003;90(5):580-8.
Flin R, Patey R. Non-technical skills for anaesthetists: developing and applying ANTS. Best Pract Res Clin Anaesthesiol. 2011;25(2):215-27.
Cook TM, Woodall N, Harper J, Benger J, Fourth National Audit P. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011;106(5):632-42.
Jones CPL, Fawker-Corbett J, Groom P, Morton B, Lister C, Mercer SJ. Human factors in preventing complications in anaesthesia: a systematic review. Anaesthesia. 2018;73 Suppl 1:12-24.
Asanathong N, Jiamjira-anon N, Eiamcharoenwit J, Mantaga S, Thanakiattiwibun C, Siriussawakul A, et al. Incidence of adverse perioperative airway complications in obese non-pregnant and pregnant patients undergoing general anesthesia. Siriraj Medical Journal. 2022;74(3):178-84.
Raksamani K, Jirativanont T, Sareenun P. Correlation of medical knowledge and non-technical skills assessment in anesthesia residents. Siriraj Medical Journal. 2020;72(6):483-7.
Oofuvong M, Pattaravit N, Kanjanawanichkul O, Siripruekpong S, Nuanjun K, Suwannarat B. Are technical skills assessed using medical knowledge associated with non-technical skill knowledge in anaesthesia resident training?. Siriraj Medical Journal. 2022;74(12):844-56. Siriraj Medical Journal. 2022;74(12):844-56.
Flin R, Fioratou E, Frerk C, Trotter C, Cook TM. Human factors in the development of complications of airway management: preliminary evaluation of an interview tool. Anaesthesia. 2013;68(8):817-25.
Shruthi AH, Dinakara D, Chandrika YR. Role of videolaryngoscope in the management of difficult airway in adults: A survey. Indian J Anaesth. 2020;64(10):855-62.
Niven AS, Doerschug KC. Techniques for the difficult airway. Curr Opin Crit Care. 2013;19(1):9-15.
Hur M, Kim JY, Min SK, Lee K, Won YJ, Kim JE. Comparison of McGrath Videolaryngoscope and Macintosh Laryngoscope in Children with Torticollis: Randomized Controlled Trial. Children (Basel). 2021;8(12).
Jones L, Mulcahy K, Fox J, Cook TM, Kelly FE. C-MAC((c)) videolaryngoscopy: The anaesthetic assistant's view. J Perioper Pract. 2018;28(4):83-9.
Edelman DA, Perkins EJ, Brewster DJ. Difficult airway management algorithms: a directed review. Anaesthesia. 2019;74(9):1175-85.
De Jong A, Myatra SN, Roca O, Jaber S. How to improve intubation in the intensive care unit. Update on knowledge and devices. Intensive Care Med. 2022;48(10):1287-98.
Herbstreit F, Fassbender P, Haberl H, Kehren C, Peters J. Learning endotracheal intubation using a novel videolaryngoscope improves intubation skills of medical students. Anesth Analg. 2011;113(3):586-90.
Malito ML, Mathias L, Kimura Junior A, Correa GH, Bardauil VR. The impact of introducing a videolaryngoscope in the initial training of laryngoscopy for undergraduate medical students: a simulation randomized trial. Braz J Anesthesiol. 2023;73(5):532-8.
Gordon M, Darbyshire D, Baker P. Non-technical skills training to enhance patient safety: a systematic review. Med Educ. 2012;46(11):1042-54.
Arora S, Miskovic D, Hull L, Moorthy K, Aggarwal R, Johannsson H, et al. Self vs expert assessment of technical and non-technical skills in high fidelity simulation. Am J Surg. 2011;202(4):500-6.
Hernan MA, Hernandez-Diaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15(5):615-25.
Park HR, Lee JS. Induced interpretation bias affects free recall and episodic memory bias in social anxiety. PLoS One. 2023;18(11):e0289584.
Additional Files
Published
How to Cite
Issue
Section
Categories
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









