
Frailty and Upper Gastrointestinal Surgery: Initial Findings from Thailand’s First Surgical Frailty Study
DOI:
https://doi.org/10.33192/smj.v77i8.276025Keywords:
Frailty, Thai frailty index, Upper gastrointestinal surgery, Postoperative complication, Perioperative mortalityAbstract
Objective: Thailand’s aging population has led to an increase in elderly patients undergoing major surgery. Frailty is a key predictor of adverse surgical outcomes, but its impact in Thai patients remains underreported. This study aimed to determine the prevalence of frailty and its association with short-term postoperative outcomes among patients undergoing upper gastrointestinal (UGI) surgery.
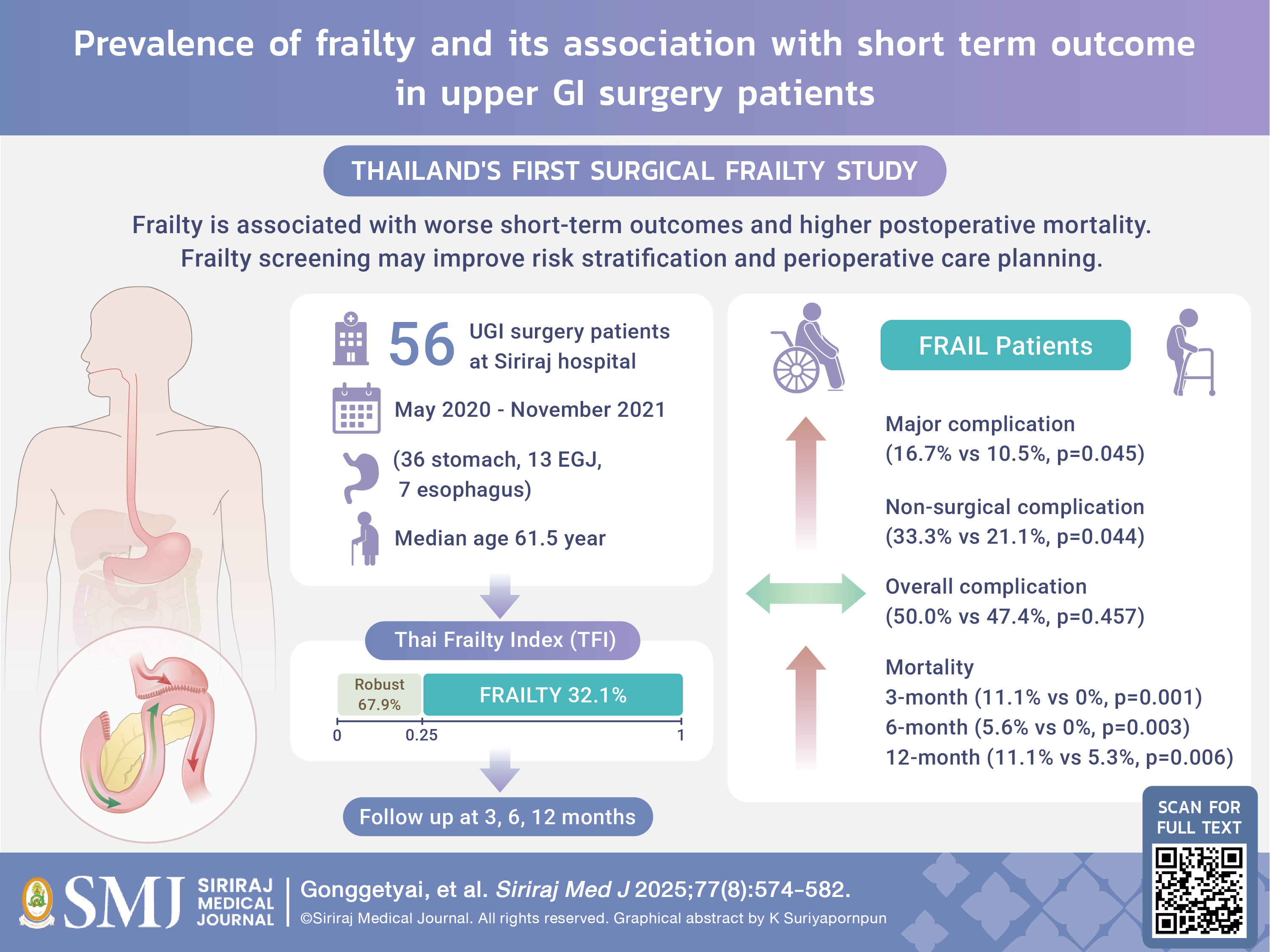
Materials and Methods: This prospective cohort study included all adult patients undergoing elective UGI surgery at Siriraj Hospital between May 2020 and November 2021. Preoperative frailty was assessed using the Thai Frailty Index (TFI), with scores >0.25 indicating frailty. Demographic data, surgical details, and postoperative outcomes—including complications and survival at 3, 6, and 12 months—were compared between frail and robust groups.
Results: Among 56 patients (median age 61.5 years), 18 (32.1%) were classified as frail. Frail patients were significantly older and had poorer functional status and nutritional risk. Frail patients also underwent fewer resection procedures (61.1% vs 84.2%, p=0.001). While the overall complication rate did not differ significantly between groups (50.0% vs 47.4%; p=0.457), frail patients experienced higher rates of major complications (16.7% vs 10.5%; p=0.045) and non-surgical complications (33.3% vs 21.1%; p=0.044). Mortality was significantly higher in the frail group at 3, 6, and 12 months postoperatively (p=0.001, 0.003, and 0.006, respectively).
Conclusion: Frailty is common among Thai patients undergoing UGI surgery and is associated with worse short-term outcomes and higher postoperative mortality. Routine frailty screening using the TFI may improve preoperative risk stratification and perioperative care planning.
References
Rønning B, Wyller TB, Nesbakken A, Skovlund E, Jordhory MS, Bakka A, et al. Quality of life in older and frail patients after surgery for colorectal cancer-A follow-up study. J Geriatr Oncol. 2016;7(3):195-200.
Xue QL. The frailty syndrome: definition and natural history. Clin Geriatr Med. 2011;27(1):1-15.
Srinonprasert V, Chalermsri C, Aekplakorn W. Frailty index to predict all-cause mortality in Thai community-dwelling older population: A result from a National Health Examination Survey cohort. Arch Gerontol Geriatr. 2018;77:124-8.
McIsaac DI, Jen T, Mookerji N, Patel A, Lalu MM. Interventions to improve the outcomes of frail people having surgery: a systematic review. PLoS ONE. 2017;12(12):e0190071.
Hodari A, Hammoud ZT, Borgi JF, Tsiouris A, Rubinfeld IS. Assessment of morbidity and mortality after esophagectomy using a modified frailty index. Ann Thorac Surg. 2013;96:1240–5.
Choe YR, Joh JY, Kim YP. Association between frailty and readmission within one year after gastrectomy in older patients with gastric cancer. J Geriatr Oncol. 2017;8(3):185-9.
Lu J, Zheng H-L, Li P, Xie J-W, Wang J-B, Lin J-X, et al. High preoperative modified frailty index has a negative impact on short- and long-term outcomes of octogenarians with gastric cancer after laparoscopic gastrectomy. Surg Endosc. 2018;32:2193–200.
Lin H-S, Watts JN, Peel NM, Hubbard RE. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157.
McIsaac DI, Taljaard M, Bryson GL, Beaulé PE, Gagné S, Hamilton G, et al. Frailty as a predictor of death or new disability after surgery: a prospective cohort study. Ann Surg. 2020;271(2):283–9.
Revenig LM, Canter DJ, Kim S, Liu Y, Sweeney JF, Sarmiento JM, et al. Report of a simplified frailty score predictive of short-term postoperative morbidity and mortality. J Am Coll Surg. 2015;220(5):904–11.
Buettner S, Wagner D, Kim Y, Margonis GA, Makary MA, Wilson A, et al. Inclusion of sarcopenia outperforms the modified frailty index in predicting 1-year mortality among 1,326 patients undergoing gastrointestinal surgery for a malignant indication. J Am Coll Surg. 2016;222(4):397–407.
Aucoin SD, Hao M, Sohi R, Shaw J, Bentov I, Walker D, et al. Accuracy and feasibility of clinically applied frailty instruments before surgery: a systematic review and meta-analysis. Anesthesiology. 2020;133(1)78-95.
Shen Y, Hao Q, Zhou J, Dong B. The impact of frailty and sarcopenia on postoperative outcomes in older patients undergoing gastrectomy surgery: a systematic review and meta-analysis. BMC Geriatr. 2017;17:188.
Mazzola M, Bertoglio C, Boniardi M, Magistro C, De Martini P, Carnevali P, et al. Frailty in major oncologic surgery of upper gastrointestinal tract: How to improve postoperative outcomes. Eur J Surg Oncol. 2017;43:1566-71.
Lu J, Cao L-L, Zheng C-H, Li P, Xie J-W, Wang J-B, et al. The Preoperative Frailty Versus Inflammation-Based Prognostic Score: Which is Better as an Objective Predictor for Gastric Cancer Patients 80 Years and Older? Ann Surg Oncol. 2017;24:754–62.
Tanaka T, Suda K, Inaba K, Umeki Y, Gotoh A, Ishida Y, et al. Impact of Frailty on Postoperative Outcomes for Laparoscopic Gastrectomy in Patients Older than 80 Years. Ann Surg Oncol. 2019;26:4016–26.
Chen FF, Zhang F-Y, Zhou X-Y, Shen X, Yu Z, Zhuang C-L, et al. Role of frailty and nutritional status in predicting complications following total gastrectomy with D2 lymphadenectomy in patients with gastric cancer: a prospective study. Langenbecks Arch Surg. 2016;401(6):813-22.
Tegels JJ, Maat MFG, Hulsewe KWE, Hoofwijk AGM, Stoot JHMB. Value of geriatric frailty and nutritional status assessment in predicting postoperative mortality in gastric cancer surgery. J Gastrointest Surg. 2014;18:439–46.
Schlitzkus LL, Melin AA, Johanning JM, Schenarts PJ. Perioperative Management of Elderly Patients. Surg Clin North Am. 2015;95(2):391-415.
Mörgeli R, Scholtz K, Kurth J, Treskatsch S, Neuner B, Koch S, et al. Perioperative Management of Elderly Patients with Gastrointestinal Malignancies: The Contribution of Anesthesia. Visc Med. 2017;33(4):267-74.
Sandrucci S, Beets G, Braga M, Dejong K, Demartines N. Perioperative nutrition and enhanced recovery after surgery in gastrointestinal cancer patients. A position paper by the ESSO task force in collaboration with the ERAS society (ERAS coalition). Eur J Surg Oncol. 2018;44(4):509-14.
Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606-17.
Dorcaratto D, Grande L, Pera M. Enhanced recovery in gastrointestinal surgery: upper gastrointestinal surgery. Dig Surg. 2013;30:70–78.
Low DE, Allum W, Manzoni G, Ferri L, Immanuel A, Kuppusamy M, et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J Surg. 2019;43:299–330.
Mortensen K, Nilsson M, Slim K, Schafer M, Mariette C, Braga M, et al. Consensus guidelines for enhanced recovery after gastrectomy Enhanced Recovery After Surgery (ERAS) Society recommendations. BJS. 2014;101:1209–29.
Parakonthun T, Tawantanakorn T, Swangsri J, Suwatthanarak T, Srisuworanan N, Taweerutchana V, et al. Results of an enhanced recovery after surgery protocol for upper gastrointestinal surgery at a super-tertiary referral hospital in Thailand. Surgery, Gastroenterology and Oncology. 2020;25(5):248-59.
Nampoolsuksan C, Parakonthun T, Tawantanakorn T, Mora A, Swangsri J, Akaraviputh T, et al. Short-term Postoperative Outcomes Before and After the Establishment of the Siriraj Upper Gastrointestinal Cancer Center: A Propensity Score Matched Analysis. Siriraj Med J. 2020;72(4):215-320.
Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin. 2017;67:93-99.
Kondrup J, Rasmussen HH, Hamberg O, Stanga Z, Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003;22:321-36.
Komindr S, Tangsermwong T, Janepanish P. Simplified malnutrition tool for Thai patients. Asia Pac J Clin Nutr. 2013;22:516-21.
Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-13.
Gu C, Lu A, Lei C, Wu Q, Zhang X, Wei M, et al. Frailty index is useful for predicting postoperative morbidity in older patients undergoing gastrointestinal surgery: a prospective cohort study. BMC Surg. 2022;22(1):57.
WHOQOL Group. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Quality of Life Research. 1993;2(2):153-9.
Papathanasiou IV, Rsmmoginni A, Papagiannis D, Malli F, Mantzaris DC, Tsaras K, et al. Frailty and Quality of Life Among Community-Dwelling Older Adults. Cureus. 2021;13(2):e13049.
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292-8.
Heng G, Lohsiriwat V, Tan K-Y. Suitability of Enhanced Recovery after Surgery (ERAS) Protocols for Elderly Colorectal Cancer Patients. Siriraj Med J. 2019;72(1):18-23.
Wang D, Kong Y, Zhong B, Zhou X, Zhou Y. Fast-track surgery improves postoperative recovery in patients with gastric cancer: a randomized comparison with conventional postoperative care. J Gastrointest Surg. 2010;14(4):620-7.
Dalton A, Zafirova Z. Preoperative Management of the Geriatric Patient: Frailty and Cognitive Impairment Assessment. Anesthesiol Clin. 2018;36:599-614.
Ko FC. Preoperative Frailty Evaluation: A Promising Risk-stratification Tool in Older Adults Undergoing General Surgery. Clin Ther. 2019;41:387-99.
Tawantanakorn T, Phibalyart W, Parakonthun T, Nampoolsuksan C, Suwatthanarak T, Srisuworanan N, et al. Changes in Physical Components after Gastrectomy for Adenocarcinoma of Stomach and Esophagogastric Junction. Siriraj Med J. 2023;75(4):241–9.
Parakonthun T, Gonggetyai G, Nampoolsuksan C, Suwatthanarak T, Tawantanakorn T, Swangsri J, et al. Higher compliance with the enhanced recovery after surgery protocol improves postoperative recovery and 6-month mortality in upper gastrointestinal surgery. Surg Pract Sci. 2024;19:100265.
Hulzebos EH, van Meeteren NL. Making the elderly fit for surgery. Br J Surg. 2016;103:e12-e15.
Somnuke P, Pongraweewan O, Siriussawakul A. Optimizing Perioperative Care for Elderly Surgical Patients: A Review of Strategies and Evidence-Based Practices. Siriraj Med J. 2024; 76(7):465-72.
Published
How to Cite
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









