
Perioperative Hypothermia in Neonates and Infants: An Update on Monitoring, Warming Strategies, and Implementation of Current Guidelines
DOI:
https://doi.org/10.33192/smj.v77i10.276540Keywords:
Perioperative hypothermia, pediatric, Anesthesia, Guideline, Warming methodsAbstract
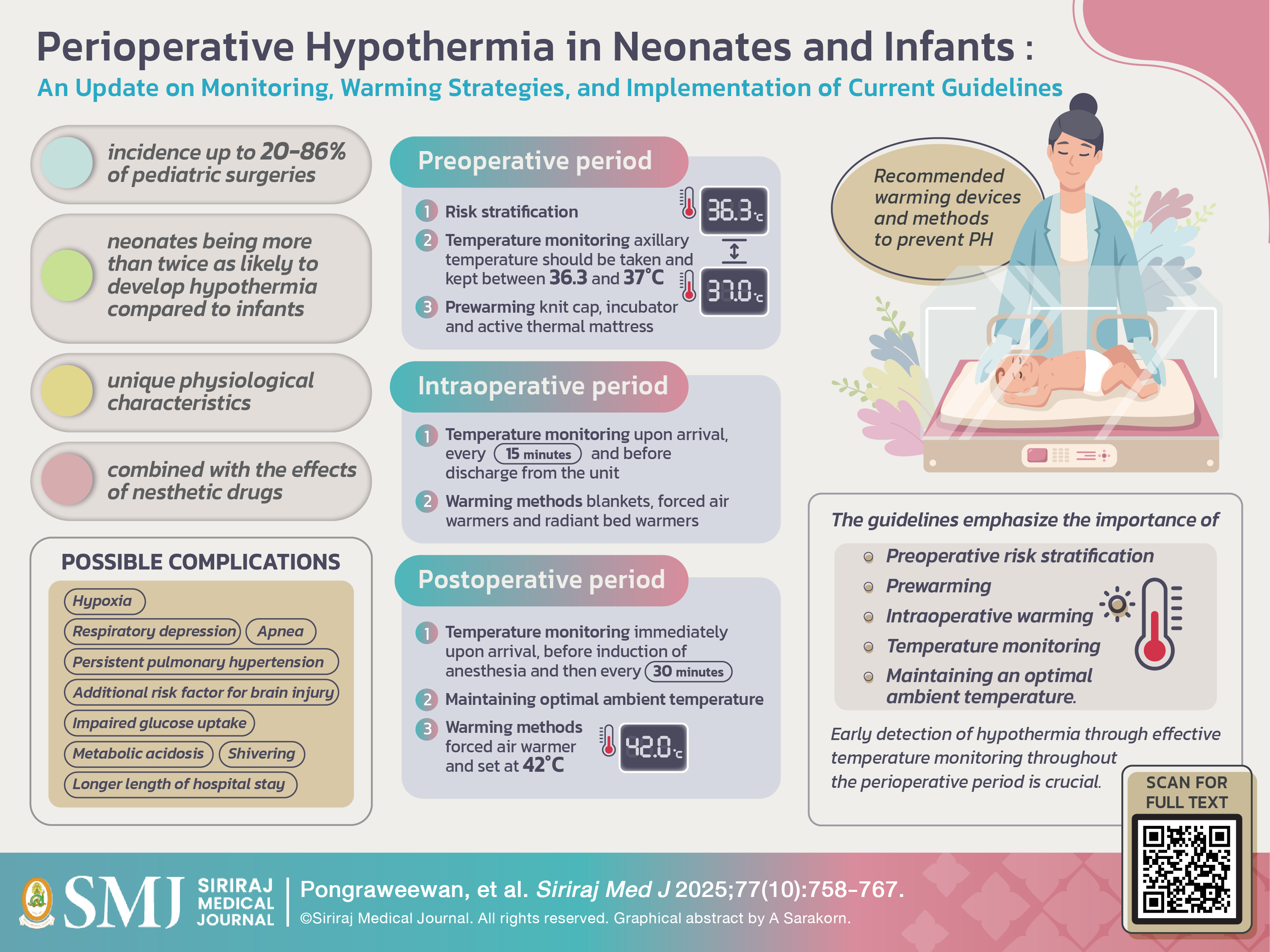
Perioperative hypothermia (PH) is a common concern in neonates and infants, and neonates are more than twice as likely to develop hypothermia due to their unique physiological characteristics. Combined with the effects of anesthetic drugs, these factors make them particularly susceptible to heat loss. Despite the implementation of effective warming methods, maintaining normothermia in this vulnerable population remains challenging. Several guidelines tailored to specific hospitals and institutions aimed to emphasize the importance of preoperative risk stratification, prewarming, intraoperative warming, temperature monitoring, and maintaining an optimal ambient temperature. Early detection of hypothermia through effective temperature monitoring throughout the perioperative period is crucial. Combining the use of warming devices with specific techniques is more effective in reducing perioperative hypothermia. This article highlights recent updates in monitoring and warming strategies, comparing the advantages and disadvantages of different approaches, and reviews the guidelines designed to prevent perioperative hypothermia in neonates and infants in order to optimize surgical outcomes.
References
Nemeth M, Miller C, Brauer A. Perioperative Hypothermia in Children. Int J Environ Res Public Health. 2021;18(14).
Zhao J, Le Z, Chu L, Gao Y, Zhang M, Fan J, et al. Risk factors and outcomes of intraoperative hypothermia in neonatal and infant patients undergoing general anesthesia and surgery. Front Pediatr. 2023;11:1113627.
Eltun Guliyev CŞ, Canan Bor, Meltem Uyar. Newborns are Prone to More Hypothermia in the Low Temperature of Operating Rooms. J Pediatr Res. 2024;11(1):30-7.
Riley C, Andrzejowski J. Inadvertent perioperative hypothermia. BJA Educ. 2018;18(8):227-33.
Kurz A, Sessler DI, Annadata R, Dechert M, Christensen R, Bjorksten AR. Midazolam Minimally Impairs Thermoregulatory Control. Anesthesia & Analgesia. 1995;81(2):393-8.
Frank SM, Beattie C, Christopherson R, Norris EJ, Rock P, Parker S, et al. Epidural versus general anesthesia, ambient operating room temperature, and patient age as predictors of inadvertent hypothermia. Anesthesiology. 1992;77(2):252-7.
Pearce B, Christensen R, Voepel-Lewis T. Perioperative Hypothermia in the Pediatric Population: Prevalence, Risk Factors and Outcomes. Journal of Anesthesia & Clinical Research. 2010;01.
Sultana R, Allen JC, Siow YN, Bong CL, Lee SY. Development of local guidelines to prevent perioperative hypothermia in children: a prospective observational cohort study. Canadian Journal of Anesthesia/Journal canadien d'anesthésie. 2022;69(11):1360-74.
Bissonnette B, Sessler DI, LaFlamme P. Intraoperative Temperature Monitoring Sites in Infants and Children and the Effect of Inspired Gas Warming on Esophageal Temperature. Anesthesia & Analgesia. 1989;69(2):192-6.
Grant Geissler M, FACS, FAAP, Thomas Moroney, MD, . Perioperative Thermoregulation. 2022.
Lodha R, Mukerji N, Sinha N, Pandey RM, Jain Y. Is axillary temperature an appropriate surrogate for core temperature? Indian J Pediatr. 2000;67(8):571-4.
Friedrichs J, Staffileno BA, Fogg L, Jegier B, Hunter R, Portugal D, et al. Axillary Temperatures in Full-Term Newborn Infants: Using Evidence to Guide Safe and Effective Practice. Advances in Neonatal Care. 2013;13(5):361-8.
Falzon A, Grech V, Caruana B, Magro A, Attard-Montalto S. How reliable is axillary temperature measurement? Acta Paediatrica. 2003;92(3):309-13.
Wongsripuemtet P, LR, T, S., VP, KC, KO, et al. Clinical guideline for prevention and management of perioperative hypothermia by the Royal College of Anesthesiologists of Thailand. Thai Journal of Anesthesiology. 2024;50(4):288-300.
NICE. Hypothermia: prevention and management in adults having surgery2008.
Sullivan G, Spencer M. Heat and temperature. BJA Education. 2022;22(9):350-6.
Kiya T, Yamakage M, Hayase T, Satoh J-I, Namiki A. The Usefulness of an Earphone-Type Infrared Tympanic Thermometer for Intraoperative Core Temperature Monitoring. Anesthesia & Analgesia. 2007;105(6):1688-92.
Imamura M, Matsukawa T, Ozaki M, Sessler DI, Nishiyama T, Kumazawa T. The accuracy and precision of four infrared aural canal thermometers during cardiac surgery. Acta Anaesthesiologica Scandinavica. 1998;42(10):1222-6.
Sessler DI. Perioperative Temperature Monitoring. Anesthesiology. 2021;134(1):111-8.
Pedersen C, Munch P, Kjaergaard J, Grønlykke L, Bräuer A. Accuracy of a zero-heat-flux thermometer in cardiac surgery, a prospective, multicentre, method comparison study. Scientific Reports. 2024;14(1):3169.
Sang B-H, Lee C, Lee DY. Prospective comparative analysis of noninvasive body temperature monitoring using zero heat flux technology (SpotOn sensor) compared with esophageal temperature monitoring during pediatric surgery. PLOS ONE. 2022;17(8):e0272720.
Ramjist JK, Sutthatarn P, Elliott C, Lee KS, Fecteau A. Introduction of a Warming Bundle to Reduce Hypothermia in Neonatal Surgical Patients. J Pediatr Surg. 2024;59(5):858-62.
Luginbuehl I, Bissonnette B, Davis P. Thermoregulation: Physiology and Perioperative Disturbances. 2006. p. 153-76.
Buisson P, Bach V, Elabbassi EB, Chardon K, Delanaud S, Canarelli JP, et al. Assessment of the efficiency of warming devices during neonatal surgery. European Journal of Applied Physiology. 2004;92(6):694-7.
Kim HY, Lee KC, Lee MJ, Kim MN, Kim JS, Lee WS, et al. Comparison of the efficacy of a forced-air warming system and circulating-water mattress on core temperature and post-anesthesia shivering in elderly patients undergoing total knee arthroplasty under spinal anesthesia. Korean J Anesthesiol. 2014;66(5):352-7.
Albrecht M, Gauthier RL, Belani K, Litchy M, Leaper D. Forced-air warming blowers: An evaluation of filtration adequacy and airborne contamination emissions in the operating room. Am J Infect Control. 2011;39(4):321-8.
Moretti B, Larocca AMV, Napoli C, Martinelli D, Paolillo L, Cassano M, et al. Active warming systems to maintain perioperative normothermia in hip replacement surgery: a therapeutic aid or a vector of infection? Journal of Hospital Infection. 2009;73(1):58-63.
Wadhwa A, Komatsu R, Orhan-Sungur M, Barnes P, In J, Sessler DI, et al. New Circulating-Water Devices Warm More Quickly than Forced-Air in Volunteers. Anesthesia & Analgesia. 2007;105(6):1681-7.
Erdoğan H, Işıl C, Türk H, Ergen G, Oba S. The Comparison of Forced-air Warming Systems and Intravenous Fluid Warmers in the Prevention of Pediatric Perioperative Hypothermia. Medical Bulletin of Haseki. 2019;57.
Shen J, Wang Q, Zhang Y, Wang X, Shi P. Combination of warming blanket and prewarmed intravenous infusion is effective for rewarming in infants with postoperative hypothermia in China. Paediatr Anaesth. 2015;25(11):1139-43.
Gray PH, Flenady V. Cot-nursing versus incubator care for preterm infants. Cochrane Database Syst Rev. 2003(1):Cd003062.
Matsuzaki Y, Matsukawa T, Ohki K, Yamamoto Y, Nakamura M, Oshibuchi T. Warming by resistive heating maintains perioperative normothermia as well as forced air heating. Br J Anaesth. 2003;90(5):689-91.
McCall EM, Alderdice F, Halliday HL, Vohra S, Johnston L. Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2018;2(2):Cd004210.
Bissonnette B, Sessler Daniel I, LaFlamme P. Passive and Active Inspired Gas Humidification in Infants and Children. Anesthesiology. 1989;71(3):350-4.
Bell GT, Martin KM, Beaton S. Work of breathing in anesthetized infants increases when a breathing system filter is used. Paediatr Anaesth. 2006;16(9):939-43.
Published
How to Cite
Issue
Section
Categories
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









