
Diagnostic Utility of Reticulocyte Hemoglobin Equivalent for Identifying Iron Deficiency in Hospitalized Children in a Thalassemia-endemic Region: A Single-center Cross-sectional Study
DOI:
https://doi.org/10.33192/smj.v78i1.277456Keywords:
Anemia, children, diagnostic accuracy, hospitalization, iron deficiency, receiver operating characteristic, reticulocyte hemoglobin equivalent, thalassemiaAbstract
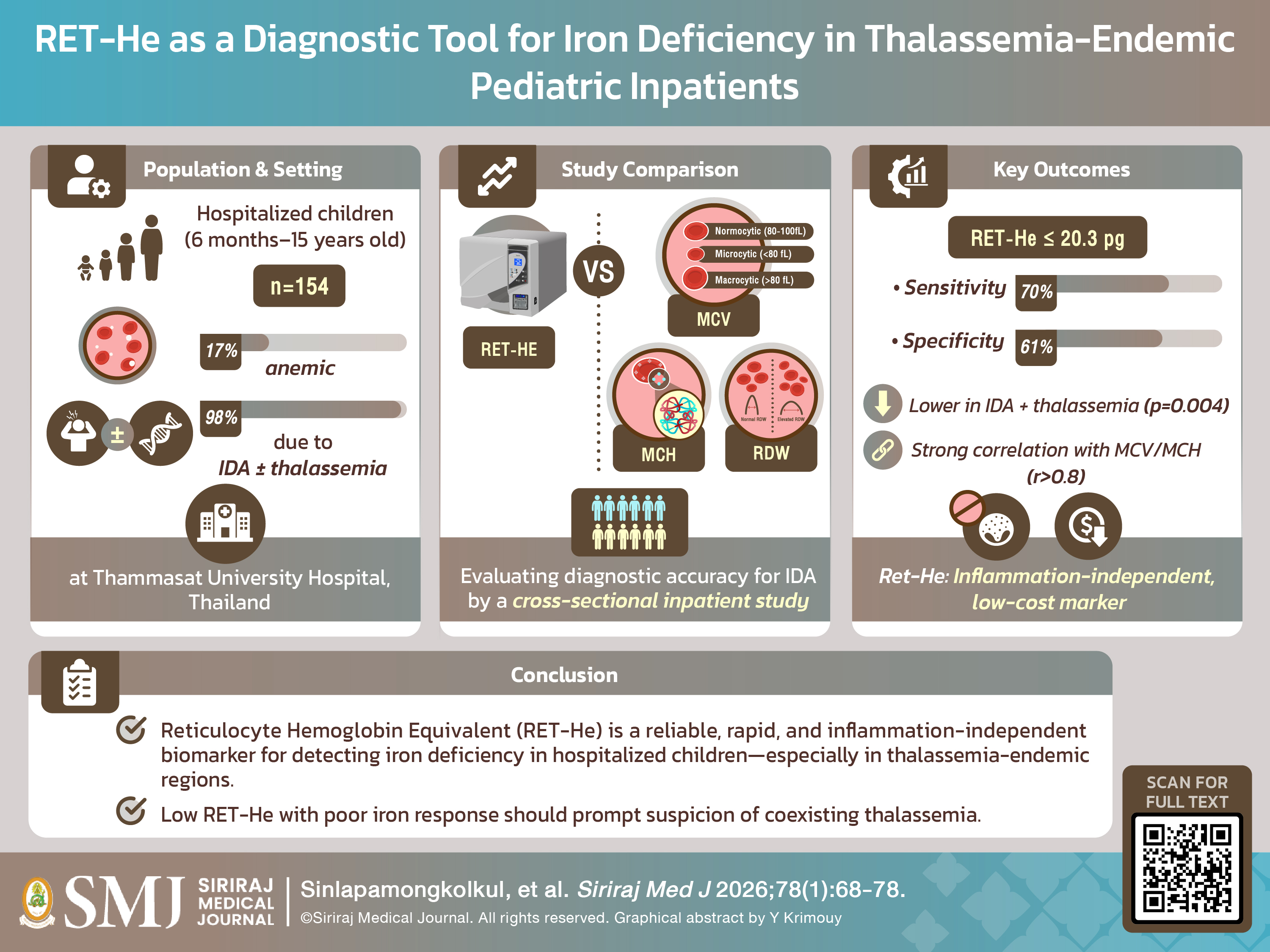
Objective: Reticulocyte hemoglobin equivalent (RET-He) has been identified as a useful marker for diagnosing and monitoring iron deficiency anemia (IDA). This study evaluated anemia prevalence and assessed RET-He’s effectiveness in detecting IDA in pediatric inpatients with high thalassemia burden.
Materials and Methods: A cross-sectional design was employed involving children aged 6 months to 15 years admitted with anemia. RET-He and red blood cell (RBC) indices were compared to explore diagnostic implications.
Results: Among the 881 pediatric inpatients included during the study period, 17% (154 patients) were identified as having anemia. IDA was the major cause of anemia (98%), including IDA (70.1%) and IDA coexisting with thalassemia (27.9%). Median RET-He (IQR) of all anemic patients was 21.05 (18.70, 24) pg. Notably, RET-He values were lower in patients with combined IDA and thalassemia than in those with IDA alone (p = 0.004). Significant correlations were observed between RET-He and RBC indices such as mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH). With a cut-off of ≤20.3 pg, RET-He showed moderate sensitivity (70.3%) and specificity (60.5%) for diagnosing IDA.
Conclusion: These findings advocate for RET-He’s use as an iron status marker in hospitalized children, especially in areas endemic for thalassemia. Low RET-He in non-responders to iron therapy should raise suspicion of underlying thalassemia.
References
Bathla S, Arora S. Prevalence and approaches to manage iron deficiency anemia (IDA). Crit Rev Food Sci Nutr. 2022;62(32):8815-28.
Moscheo C, Licciardello M, Samperi P, La Spina M, Di Cataldo A, Russo G. New Insights into Iron Deficiency Anemia in Children: A Practical Review. Metabolites. 2022;12(4):289.
Angeles IT, Schultink WJ, Matulessi P, Gross R, Sastroamidjojo S. Decreased rate of stunting among anemic Indonesian preschool children through iron supplementation. Am J Clin Nutr. 1993;58(3):339-42.
Lozoff B, Beard J, Connor J, Barbara F, Georgieff M, Schallert T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr Rev. 2006;64(5 Pt 2):S34-43; discussion S72-91.
Mei Z, Addo OY, Jefferds MED, Sharma AJ, Flores-Ayala RC, Pfeiffer CM, Brittenham GM. Comparison of Current World Health Organization Guidelines with Physiologically Based Serum Ferritin Thresholds for Iron Deficiency in Healthy Young Children and Nonpregnant Women Using Data from the Third National Health and Nutrition Examination Survey. J Nutr. 2023;153(3):771-80.
Johnson-Wimbley TD, Graham DY. Diagnosis and management of iron deficiency anemia in the 21st century. Therap Adv Gastroenterol. 2011;4(3):177-84.
Mateos ME, De-la-Cruz J, López-Laso E, Valdés MD, Nogales A. Reticulocyte hemoglobin content for the diagnosis of iron deficiency. J Pediatr Hematol Oncol. 2008;30(7):539-42.
Ogawa C, Tsuchiya K, Maeda K. Reticulocyte hemoglobin content. Clin Chim Acta. 2020;504:138-45.
Fucharoen S, Winichagoon P. Haemoglobinopathies in southeast Asia. Indian J Med Res. 2011;134(4):498-506.
Leckngam, P. Thalassemia and Hemoglobinopathies in Thailand: A Systematic Review. J Health Sci Altern Med. 2023;5(3):104-13.
Sedick Q, Elyamany G, Hawsawi H, Alotaibi S, Alabbas F, Almohammadi M, et al.
Diagnostic accuracy of reticulocyte parameters on the Sysmex XN 1000 for
discriminating iron deficiency anaemia and thalassaemia in Saudi Arabia. Am J
Blood Res. 2021;11(2):172-9.
Kadegasem P, Songdej D, Lertthammakiat S, Chuansumrit A, Paisooksantivatana
K, Mahaklan L, et al. Reticulocyte hemoglobin equivalent in a thalassemia-prevalent area. Pediatr Int. 2019;61(3):240-5.
Rohr M, Brandenburg V, Brunner-La Rocca HP. How to diagnose iron deficiency in chronic disease: A review of current methods and potential marker for the outcome. Eur J Med Res. 2023;28:15.
Lee NH. Iron deficiency in children with a focus on inflammatory conditions. Clin Exp Pediatr. 2024;67(6):283-93.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377-81.
World Health Organization. WHO Anthro for personal computers, version 3.2.2, 2011: Software for assessing growth and development of the world's children. Geneva: WHO, 2010. [cited 2024 Apr 30]. Available from: https://www.who.int/childgrowth/software/en/
World Health Organization. WHO AnthroPlus for personal computers manual: software for assessing growth of the world's children and adolescents. Geneva: WHO; 2009. [cited 2024 Apr 30]. Available from: https://www.who.int/growthref/tools/en/
Eng B PM, Walker L, Chui DHK, Waye JS. Detection of severe nondeletional α-thalassemia mutations using a single-tube multiplex ARMS assay. Genet Test. 2001;5:327-9.
Newton CR, Graham A, Heptinstall LE, Powell SJ, Summers C, Kalsheker N, et al. Analysis of any point mutation in DNA. The amplification refractory mutation system (ARMS). Nucleic Acids Research. 1989;17(7):2503–16.
World Health Organization. Iron deficiency anemia: assessment, prevention and control. A guide for programme managers. Geneva, World Health Organization; 2001.
Tantawy AA, Ragab IA, Ismail EA, Ebeid FSE, Al-Bshkar RM. Reticulocyte Hemoglobin Content (Ret He): A Simple Tool for Evaluation of Iron Status in Childhood Cancer. J Pediatr Hematol Oncol. 2020;42(3):e147-51.
Syed S, Kugathasan S, Kumar A, Prince J, Schoen BT, McCracken C, et al. Use of Reticulocyte Hemoglobin Content in the Assessment of Iron Deficiency in Children With Inflammatory Bowel Disease. J Pediatr Gastroenterol Nutr. 2017;64(5):713-20.
Camaschella C. Iron deficiency: new insights into diagnosis and treatment. Hematology Am Soc Hematol Educ Program. 2015;2015:8-13.
Tritipsombut J, Phylipsen M, Viprakasit V, Chalaow N, Sanchaisuriya K, Giordano PC, et al. A single-tube multiplex gap-polymerase chain reaction for the detection of eight beta-globin gene cluster deletions common in Southeast Asia. Hemoglobin. 2012;3:571-80.
Craig JE, Barnetson RA, Prior J, Raven JL, Thein SL. Rapid detection of deletions caused β-thalassemia and hereditary persistence of fetal hemoglobin by enzymatic amplification. Blood. 1994;83:1673-82.
Lian Y, Shi J, Nie N, Huang Z, Shao Y, Zhang J, et al. Reticulocyte Hemoglobin Equivalent (Ret-He) Combined with Red Blood Cell Distribution Width Has a Differentially Diagnostic Value for Thalassemias. Hemoglobin. 2019;43(4-5):229-35.
Jamnok J, Sanchaisuriya K, Chaitriphop C, Sanchaisuriya P, Fucharoen G,
Fucharoen S. A New Indicator Derived From Reticulocyte Hemoglobin Content for
Screening Iron Deficiency in an Area Prevalent for Thalassemia. Lab Med. 2020;51(5):498-506.
Khorwanichakij N, Kungwankiattichai S, Owattanapanich W. Validation of Several Formulas to Differentiate Thalassemia from Iron Deficiency Anemia and Proposal of a Thalassemia–Iron Deficiency Discrimination (TID) Predictive Score. Siriraj Med J. 2022;74(4):256-65.
Almashjary MN, Barefah AS, Bahashwan S, Ashankyty I, ElFayoumi R, Alzahrani M, et al. Reticulocyte Hemoglobin-Equivalent Potentially Detects, Diagnoses and Discriminates between Stages of Iron Deficiency with High Sensitivity and Specificity. J Clin Med. 2022;11(19):5675.
Yuan QR, Niu SQ, Lin XP, Luo ZF. The Clinical Value of Combined Detection of
RBC, Ret-He and HbA2 for Thalassemia. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2021;29(1):203-6.
Saboor M. Discrimination of Iron Deficiency, Alpha and Beta Thalassemia on
the Basis of Red Cell Distribution Width and Reticulocyte Indices. Clin Lab.
;67(6).
Published
How to Cite
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









