
Incidence and Associated Factors for Inappropriate Blood Cross Matching in Cardiovascular Thoracic Surgeries at a Tertiary Care Center: A Retrospective Study Using Binary Logistic Regression
DOI:
https://doi.org/10.33192/smj.v78i4.280517Keywords:
Inappropriate PRC cross-matching, Cardiovascular thoracic surgeries, Cross-match to transfusion ratio, Elective surgery, Pre-operative hematocrit, Intraoperative blood lossAbstract
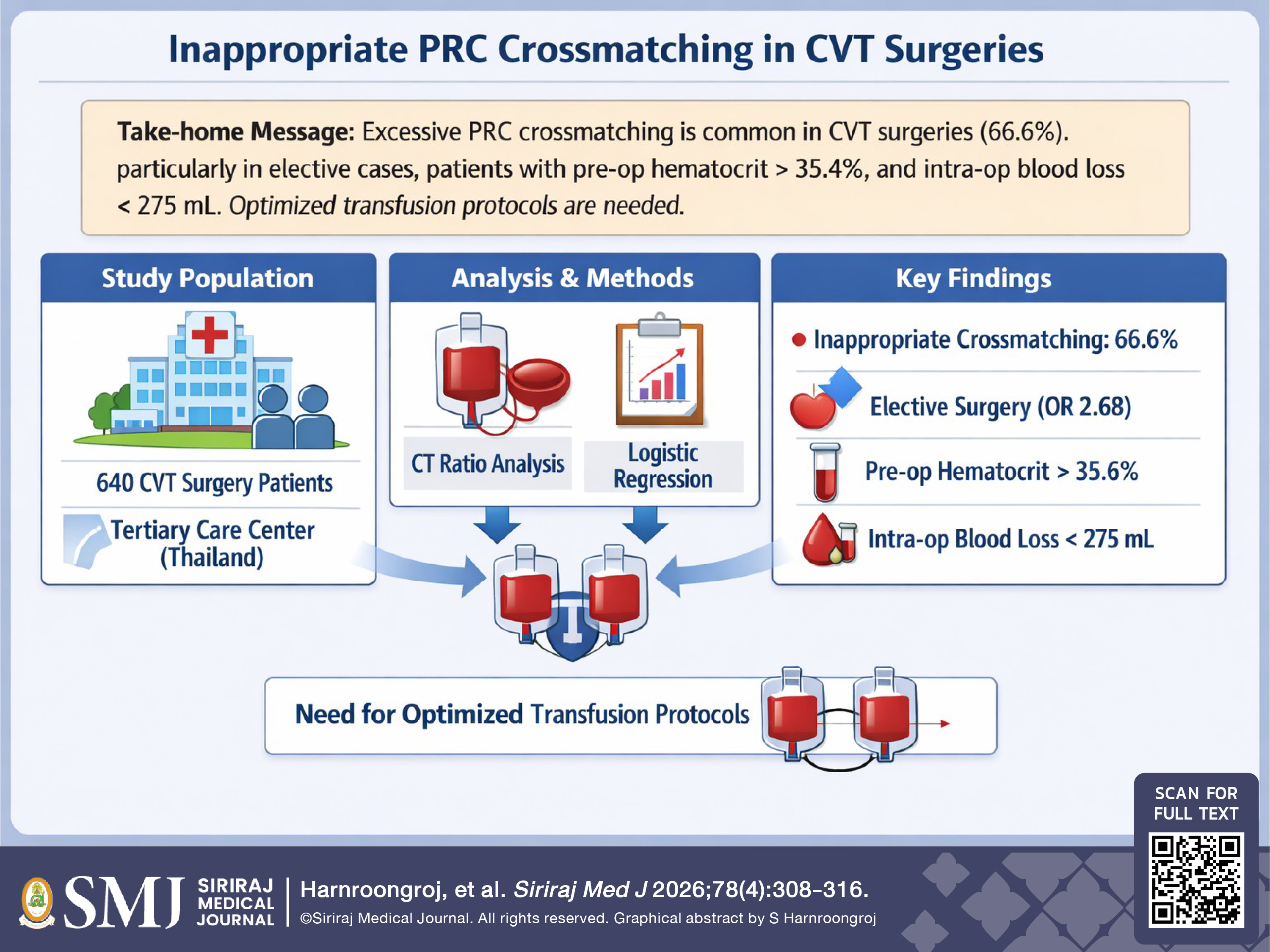
Objective: To determine the incidence of inappropriate packed red cell (PRC) crossmatching in Cardiovascular Thoracic (CVT) surgeries at a service-focused tertiary care center, and to identify the associated factors for the inappropriate PRC cross-matching.
Materials and Methods: A retrospective cross-sectional study was conducted involving 640 patients who underwent CVT surgery between 2022 and 2025. The data reviewed included the patients’ demographics, operative details, and PRC utilization (specifically, crossmatching and transfusion within 24 hours postoperatively). The crossmatch to transfusion (CT) ratio, transfusion probability (%T), and transfusion index (Ti) were calculated. An individual CT ratio > 2.0 was defined as inappropriate crossmatching. Binary logistic regression was used to identify the associated factors for inappropriate PRC crossmatching, and the Youden index to determine the optimal cutoff values.
Results: Inappropriate PRC crossmatching occurred in 426 of the 640 cases (66.6%). The overall CT ratio was 2.36, exceeding the recommended threshold limit of 2.0 and suggesting excessive blood ordering. Closed heart surgeries had the highest CT ratio (13.8), followed by thoracic surgeries (4.21). Significant factors associated with inappropriate crossmatching included elective surgery, a pre-operative hematocrit level > 35.4%, and intraoperative blood loss < 275 mL.
Conclusion: Inappropriate PRC crossmatching is common in CVT surgeries, with an incidence of 66.6% in this study cohort. Elective procedures, a higher pre-operative hematocrit level, and lower intraoperative blood loss were found to be key predictors for inappropriate PRC crossmatching. These findings highlight the need for more evidence-based transfusion protocols to minimize excessive crossmatching in CVT surgeries, and optimize the utilization of blood resources.
References
Chanthawong S, Noirit A, Khenthaiwai S, Khawnonrang L, Prakrankamanant D, Plengpanich P. Optimization of Preoperative Routine Cross-Matching for Elective Cardiothoracic Surgery in a University Hospital. Thai J Anesthesiol. 2018;44(4):157-65.
Ural KG, Volpi-Abadie J, Owen G, Gilly G, Egger AL, Scuderi-Porter H. Tailoring the Blood Ordering Process for Cardiac Surgical Cases Using an Institution-Specific Version of the Maximum Surgical Blood Order Schedule. Semin Cardiothorac Vasc Anesth. 2016;20(1):93-99.
Mangwana, Sadhana; Bedi, Neha; Yadav, Pinky; Chugh, Rakesh. Optimization of Blood Transfusion Services: Analysis of Blood Requisition and Utilization Practices in Cardiac Surgical Patients in a Tertiary Care Hospital, India. Global Journal of Transfusion Medicine. 2017;2(1):47-51.
Galata C, Roessner ED, Dette F, Conradi R, Bastuck V, Stamenovic D, et al. An update on red blood cell transfusion in non-cardiac thoracic surgery. J Thorac Dis. 2023;15(6):2926-35.
Kawattikul J. Appropriateness of Blood Preparation of Patients Underwent Elective Surgery in Mahasarakham Hospital. Thai J Anesthesiol. 2025;51(3):177-86.
Frank SM, Oleyar MJ, Ness PM, Tobian AA. Reducing unnecessary preoperative blood orders and costs by implementing an updated institution-specific maximum surgical blood order schedule and a remote electronic blood release system. Anesthesiology. 2014;121(3):501-9.
Friedman BA, Oberman HA, Chadwick AR, Kingdon KI. The maximum surgical blood order schedule and surgical blood use in the United States. Transfusion. 1976;16(4):380-7.
Fung MK, Grossman BJ, Hillyer CD, Westhoff CM. Technical manual. 18th ed. Bethesda: American Association of Blood Banks; 2014.p.227.
Chanachaisuwan P. Blood utilization in elective surgery at Police General Hospital. J Hematol Transfus Med. 2010;20:93-104.
Davoudi-kiakalayeh A, Faranoush M, Haghbin A, Behboudi F. Reviewing the blood ordering schedule in tertiary trauma center. Iranian J Blood Cancer. 2013;6:27-31.
Haghpanah S, Miladi S, Kasraian L, Zamani A, Gholami M. Blood transfusion practice in operating rooms in Nemazee Hospital in Southern Iran. Arch Iran Med. 2021;24(2):107-12.
Singh S, Kumar N, Mahla M, Sharma R, Kumar A. Maximum Surgical Blood Order Schedule (MSBOS) for Cardio-Thoracic& Vascular Interventions in an Apex Terciary Care Hospital of India. IJSR. 2021;10(11):923-6.
Ural K, Trusheim J, Amiri Y, Gastanaduy M. Improved cost-effectiveness and blood product utilization from instituting a Blood Order Algorithm for cardiac surgical cases. Semin Cardiothorac Vasc Anesth. 2018;22(4):353-8.
Siritongtaworn A, To-adithep P, Chaiwat O. The Implementation of a Red Blood Cell Transfusion Guideline in Critically Ill Surgical Patients at Siriraj Hospital. Siriraj Med J. 2019;71(1):66-73.
Published
How to Cite
License
Copyright (c) 2026 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









