
Incidence of Postoperative Residual Neuromuscular Blockade at the Postanesthesia Care Unit Following General Anesthesia
DOI:
https://doi.org/10.33192/smj.v77i7.272875Keywords:
Residual neuromuscular block, NMBAs, muscle relaxant, postanesthesia care unit, train-of-fourAbstract
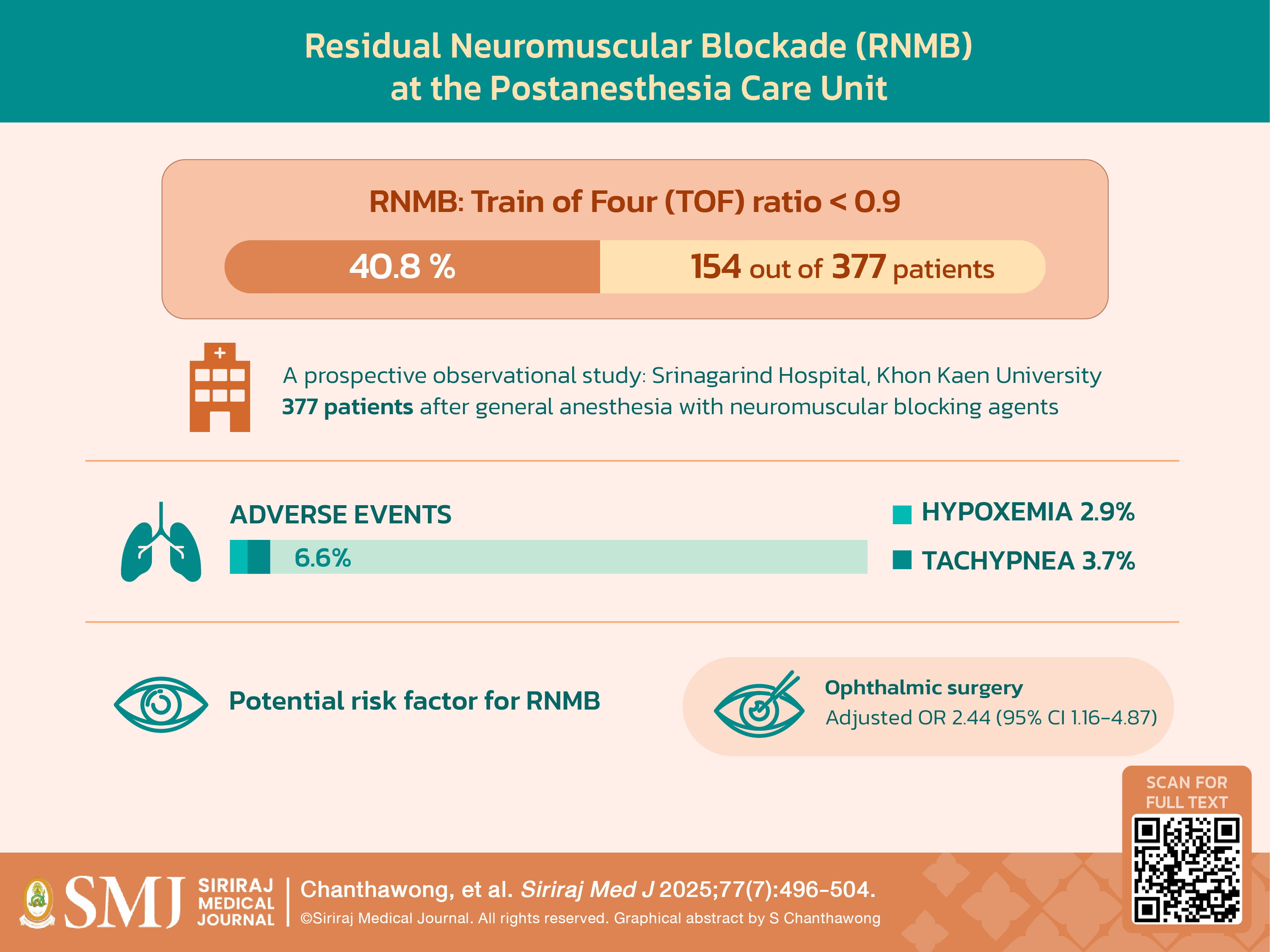
Objective: This study aimed to investigate residual neuromuscular blockade (RNMB) and respiratory adverse events and identify risk factors for RNMB.
Material and Methods: A prospective observational study enrolled 377 elective adult patients with American Society of Anesthesiologists (ASA) classifications 1–3 who underwent GA with NMBAs. At the conclusion of surgery, endotracheal tubes were removed once clinical extubation criteria were met. The Train-of-Four (TOF) ratio was immediately measured upon the patients’ arrival in the post-anesthesia care unit (PACU), with RNMB defined as a TOF ratio < 0.9. Respiratory adverse events were documented.
Results: The incidence of RNMB was 40.8% upon PACU arrival, with a median TOF ratio of 0.92 (interquartile range [IQR], 0.85–0.98). Cisatracurium was the primary NMBA used (98.1%). The incidence of respiratory adverse events was 6.6%, including hypoxemia (2.9%) and tachypnea (3.7%). No cases of reintubation or unplanned ICU admission occurred. The ophthalmologic surgery emerged as the only significant risk factor for RNMB, adjusted OR 2.44 (95% CI, 1.16-4.38, p = 0.02).
Conclusion: The incidence of RNMB after GA in the PACU was common, though no serious adverse events were observed. The type of surgery was identified as the sole significant risk factor for RNMB.
References
Baillard C, Clec’h C, Catineau J, Salhi F, Gehan G, Cupa M, et al. Postoperative residual neuromuscular block: a survey of management. Br J Anaesth. 2005;95(5):622–6.
Yu B, Ouyang B, Ge S, Luo Y, Li J, Ni D, et al. Incidence of postoperative residual neuromuscular blockade after general anesthesia: a prospective, multicenter, anesthetist-blind, observational study. Curr Med Res Opin. 2016;32(1):1–9.
Plaud B, Debaene B, Donati F, Marty J. Residual paralysis after emergence from anesthesia. Anesthesiology. 2010;112(4):1013–22.
Murphy GS, Szokol JW, Marymont JH, Greenberg SB, Avram MJ, Vender JS. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg. 2008;107(1):130–7.
Grosse-Sundrup M, Henneman JP, Sandberg WS, Bateman BT, Uribe JV, Nguyen NT, et al. Intermediate acting non-depolarizing neuromuscular blocking agents and risk of postoperative respiratory complications: prospective propensity score matched cohort study. BMJ. 2012;345:e6329.
Arbous MS, Meursing AEE, van Kleef JW, de Lange JJ, Spoormans HHAJM, Touw P, et al. Impact of anesthesia management characteristics on severe morbidity and mortality. Anesthesiology. 2005;102(2):257–68; quiz 491–2.
Butterly A, Bittner EA, George E, Sandberg WS, Eikermann M, Schmidt U. Postoperative residual curarization from intermediate-acting neuromuscular blocking agents delays recovery room discharge. Br J Anaesth. 2010;105(3):304–9.
Plaud B, Baillard C, Bourgain JL, Bouroche G, Desplanque L, Devys JM, et al. Guidelines on muscle relaxants and reversal in anaesthesia. Anaesth Crit Care Pain Med. 2020;39(1):125–42.
Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010;111(1):120–8.
Brull SJ, Murphy GS. Residual neuromuscular block: lessons unlearned. Part II: methods to reduce the risk of residual weakness. Anesth Analg. 2010;111(1):129–40.
Murphy GS. Residual neuromuscular blockade: incidence, assessment, and relevance in the postoperative period. Minerva Anestesiol. 2006;72(3):97–109.
Berg H, Roed J, Viby-Mogensen J, Mortensen CR, Engbaek J, Skovgaard LT, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997;41(9):1095–103.
Esteves S, Martins M, Barros F, Barros F, Canas M, Vitor P, et al. Incidence of postoperative residual neuromuscular blockade in the postanaesthesia care unit: an observational multicentre study in Portugal. Eur J Anaesthesiol. 2013;30(5):243–9.
Moningi S, Durga P, Mantha S, Ramachandra G. Train of Four Responses in Paretic Limbs. Journal of Neurosurgical Anesthesiology [Internet]. 2009;21(4). Available from: https://journals.lww.com/jnsa/fulltext/2009/10000/train_of_four_responses_in_paretic_limbs.9.aspx
Thongsing A, Likasitwattanakula S, Netsuwan T, Sanmaneechai O. Pediatric Neuromuscular Diseases Prevalence in Siriraj Hospital, Thailand’s Largest Tertiary Referral Hospital. Siriraj Med J. 2020;72(2):125–31.
Aytac I, Postaci A, Aytac B, Sacan O, Alay GH, Celik B, et al. Survey of postoperative residual curarization, acute respiratory events and approach of anesthesiologists. Braz J Anesthesiol. 2016;66(1):55–62.
Carvalho H, Verdonck M, Cools W, Geerts L, Forget P, Poelaert J. Forty years of neuromuscular monitoring and postoperative residual curarisation: a meta-analysis and evaluation of confidence in network meta-analysis. Br J Anaesth. 2020;125(4):466–82.
Khamtuikrua C, Suksompong S, Rhoopanwong S, Sangsab P, Chaikittisilpa N, Bormann B von. Risk Factors for Residual Neuromuscular Blockade after General Anesthesia. J Med Assoc Thai. 2017;100(Suppl 7):S75-S84.
Murphy GS, Szokol JW, Marymont JH, Greenberg SB, Avram MJ, Vender JS, et al. Intraoperative acceleromyographic monitoring reduces the risk of residual neuromuscular blockade and adverse respiratory events in the postanesthesia care unit. Anesthesiology. 2008;109(3):389–98.
Lee LA, Athanassoglou V, Pandit JJ. Neuromuscular blockade in the elderly patient. J Pain Res. 2016;9:437–44.
Murphy GS, Szokol JW, Avram MJ, Greenberg SB, Shear TD, Vender JS, et al. Residual Neuromuscular Block in the Elderly: Incidence and Clinical Implications. Anesthesiology. 2015;123(6):1322–36.
Sagir O, Yucesoy Noyan F, Koroglu A, Cicek M, Ilksen Toprak H. Comparison between the Effects of Rocuronium, Vecuronium, and Cisatracurium Using Train-of-Four and Clinical Tests in Elderly Patients. Anesth Pain Med. 2013;2(4):142–8.
Tantibhaedhyangkul P, Kuptniratsaikul V, Tosayanonda O. Grip and Quadriceps Strength: Normative Values in the Thai Population. Siriraj Med J. 2020;53(4):224–30.
Published
How to Cite
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









