
Binocular Diplopia After Cataract Surgery: Incidence and Associated Factors in a Tertiary Teaching Eye Center
DOI:
https://doi.org/10.33192/smj.v78i2.277766Keywords:
Binocular diplopia, cataract surgery, complication, risk factors, axial lengthAbstract
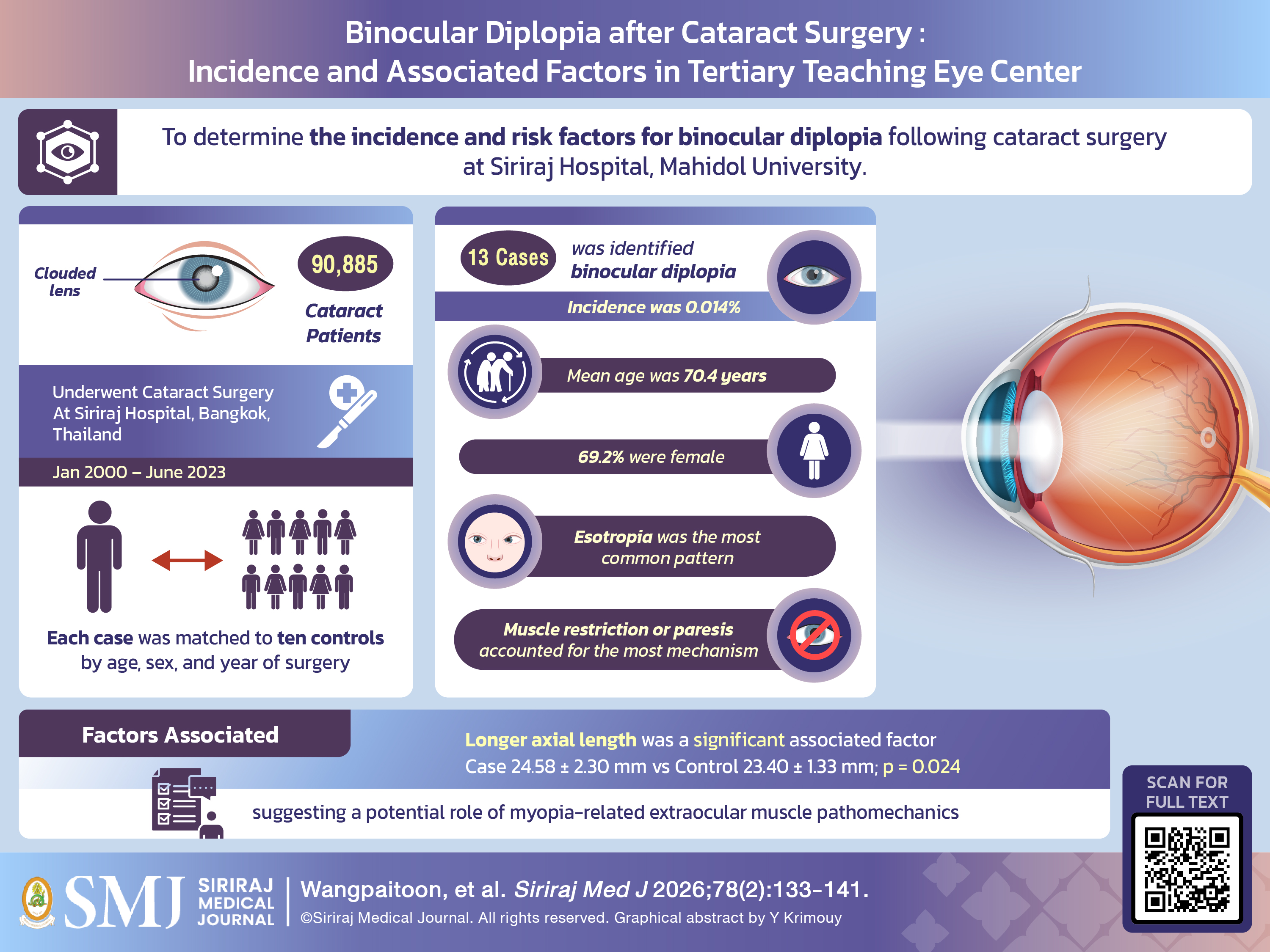
Objective: To determine the incidence and risk factors for binocular diplopia following cataract surgery at Siriraj Hospital, Mahidol University.
Materials and Methods: This retrospective case–control study included patients who underwent cataract surgery between January 2000 and June 2023. Postoperative binocular diplopia was defined as symptomatic diplopia with documented ocular misalignment within 90 days of surgery, identified using ICD-10 codes. Demographic, systemic, biometric, and operative data were extracted. Each case was matched to ten controls by age, sex, and year of surgery. Statistical analyses included Chi-square tests, paired t-tests, and logistic regression.
Results: Among 90,885 cataract surgeries, 13 cases of postoperative binocular diplopia were identified, yielding an incidence of 0.0143%, substantially lower than previously reported rates (0.18–0.85%). The mean age of affected patients was 70.4 years, and 69.2% were female. Esotropia was the most common strabismic pattern (46.2%), while muscle restriction or paresis accounted for the majority of mechanisms (53.9%). Compared with matched controls, cases had significantly longer axial lengths (24.58 ± 2.30 mm vs. 23.40 ± 1.33 mm; p = 0.024), corresponding to an odds ratio of 1.426 (95% CI: 1.047–1.942) per millimeter increase. No significant associations were found with systemic comorbidities (diabetes, hypertension, dyslipidemia) or anesthesia type.
Conclusion: Postoperative binocular diplopia following cataract surgery was rare in this large tertiary center cohort. Longer axial length was the only significant risk factor identified, suggesting a potential role of myopia-related extraocular muscle pathomechanics. Awareness of this risk factor may aid in preoperative counseling and surgical planning.
References
Han X, Zhang J, Liu Z, Tan X, Jin G, He M, Luo L, Liu Y. Real-world visual outcomes of cataract surgery based on population-based studies: a systematic review. Br J Ophthalmol. 2023;107(8):1056-65.
Kalantzis G, Papaconstantinou D, Karagiannis D, Koutsandrea C, Stavropoulou D, Georgalas I. Post-cataract surgery diplopia: aetiology, management and prevention. Clin Exp Optom. 2014;97(5):407-10.
Johnson DA. Persistent vertical binocular diplopia after cataract surgery. Am J Ophthalmol. 2001;132(6):831-5.
Pearce IA, McCready PM, Watson MP, Taylor RH. Vertical diplopia following local anaesthetic cataract surgery: predominantly a left eye problem? Eye (Lond). 2000;14(Pt 2):180–184.
Yangüela J, Gómez‑Arnau JI, Martín‑Rodrigo JC, Andueza A, Gili P, Paredes B, et al. Diplopia after cataract surgery: comparative results after topical or regional injection anesthesia. Ophthalmology. 2004;111(4):686-92.
Costa PG, Debert I, Passos LB, Polati M. Persistent diplopia and strabismus after cataract surgery under local anesthesia. Binocul Vis Strabismus Q. 2006;21(3):155-8.
Golnik KC, West CE, Kaye E, Corcoran KT, Cionni RJ. Incidence of ocular misalignment and diplopia after uneventful cataract surgery. J Cataract Refract Surg. 2000;26(8):1205-9.
Gawęcki M, Grzybowski A. Diplopia as the Complication of Cataract Surgery. J Ophthalmol. 2016;2016:2728712.
Nayak H, Kersey JP, Oystreck DT, Cline RA, Lyons CJ. Diplopia following cataract surgery: a review of 150 patients. Eye (Lond). 2008;22(8):1057–64.
Demer JL. Muscle paths matter in strabismus associated with axial high myopia. Am J Ophthalmol. 2010;149(2):184-6.e1.
Naing L, Nordin RB, Abdul Rahman H, Naing YT. Sample size calculation for prevalence studies using Scalex and ScalaR calculators. BMC Med Res Methodol. 2022;22(1):209.
Setia MS. Methodology Series Module 2: Case-control Studies. Indian J Dermatol. 2016;61(2):146-51.
Gómez‑Arnau JI, Yangüela J, González A, Andrés Y, García del Valle S, Gili P, et al. Anaesthesia‑related diplopia after cataract surgery. Br J Anaesth. 2003;90(2):189-93.
Han SK, Kim JH, Hwang J‑M. Persistent diplopia after retrobulbar anesthesia. J Cataract Refract Surg. 2004;30(6):1248-53.
Pearce IA, McCready PM, Watson MP, Taylor RH. Vertical diplopia following local anaesthetic cataract surgery: predominantly a left eye problem? Eye (Lond). 2000;14(Pt 2):180-4.
Gunton KB, Armstrong B. Diplopia in adult patients following cataract extraction and refractive surgery. Curr Opin Ophthalmol. 2010;21(5):341-4.
Rossel‑Zemkouo MJ, Bergholz R, Salchow DJ. Strabismus patterns after cataract surgery in adults. Strabismus. 2021;29(1):19-25.
Hamada S, Devys JM, Xuan TH, Ganem S, Sahel JA, Héran F, Plaud B. Role of hyaluronidase in diplopia after peribulbar anesthesia for cataract surgery. Ophthalmology. 2005;112(5):879-82.
Lin S‑C, Giang A, Liu GT, Avery RA, Shindler KS, Hamedani AG, Ross AG, Tamhankar MA. Frequency and etiologies of visual disturbance after cataract surgery identified in neuro‑ophthalmology clinics. J Neuroophthalmol. 2023;43(3):359-63.
Wylie J, Henderson M, Doyle M, Hickey-Dwyer M. Persistent binocular diplopia following cataract surgery: Aetiology and management. Eye (Lond). 1994;8:543-6.
Surachatkumtonekul T, Tongsai S, Sathianvichitr K, Sangsre P, Saiman M, Sermsripong W, et al. Corneal Curvature Change After Strabismus Surgery: An Experience from a Single Academic Center. Siriraj Med J. 2024;76(10):713-21.
Surachatkumtonekul T, Subhadhirasakul S, Sermsripong W. Visual Prognosis in Craniosynostosis Patients: A 20-year Retrospective Cohort Study at a Tertiary Referral Center in Thailand. Siriraj Med J. 2024;76(10):679-86.
ธรรมนูญ สุรชาติกำธรกุล. ภาวะตาเหล่ในผู้ป่วยสายตาสั้นมาก. ใน: ศักดิ์ชัย วงศกิตติรักษ์ ธนาพงษ์ สมกิจรุ่งโรจน์, บรรณาธิการ. จักษุวิชาการ โดย ราชวิทยาลัยจักษุแพทย์แห่งประเทศไทย เล่ม 7. กรุงเทพฯ: โรงพิมพ์มหาวิทยาลัยธรรมศาสตร์; 2566. หน้า 153-66. (In Thai)
Published
How to Cite
License
Copyright (c) 2026 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









