
Emergent Hemodialysis Initiation: A Marker of Suboptimal Pre-Dialysis Care Rather Than an Independent Predictor of Mortality
DOI:
https://doi.org/10.33192/smj.v78i2.278277Keywords:
hemodialysis initiation, unplanned start, emergency start, mortality, Thailand, ESRDAbstract
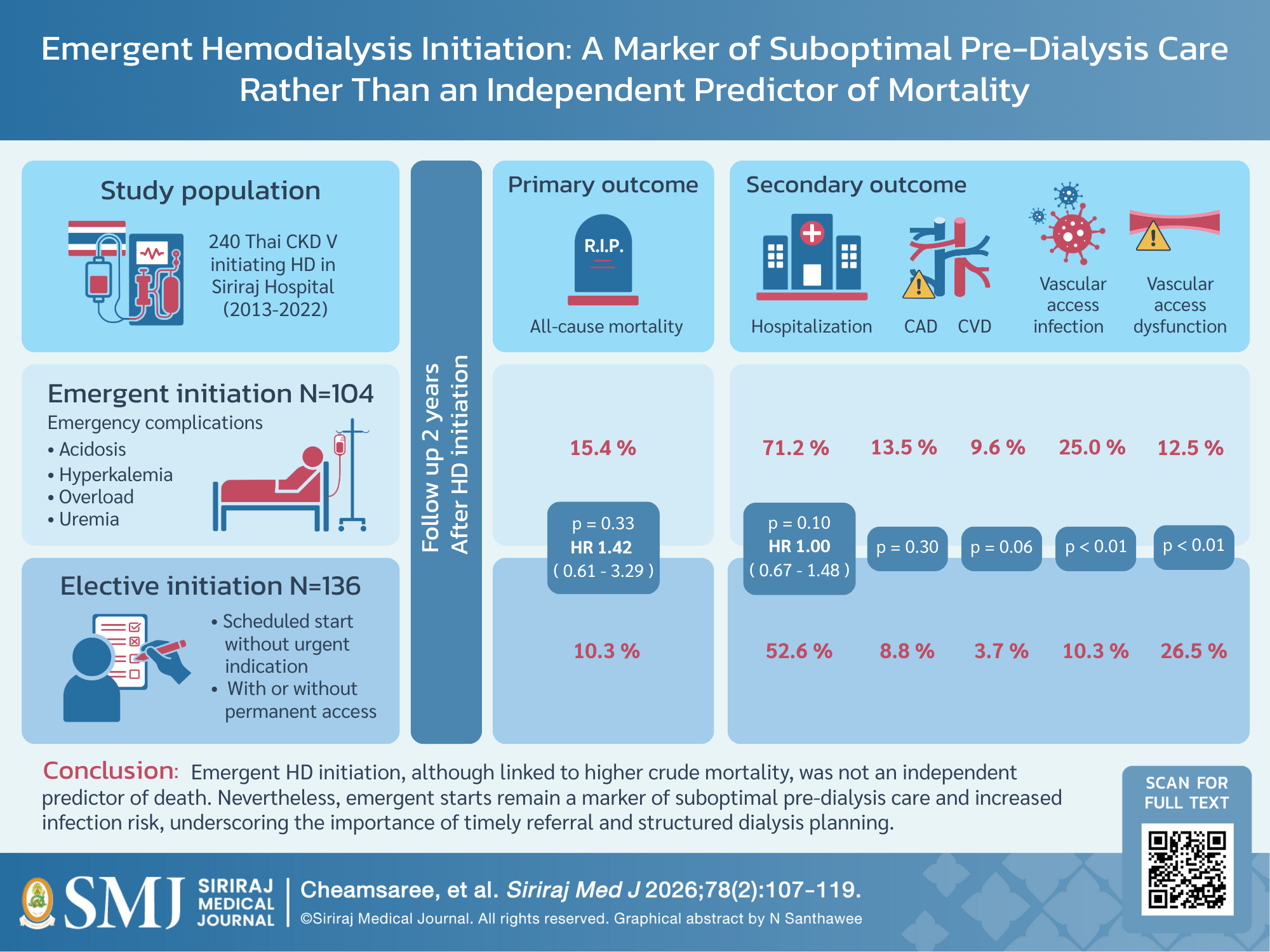
Objective: Emergent hemodialysis (HD) initiation has been consistently linked to higher mortality in prior studies, but evidence from Thailand is limited. This study evaluated the impact of elective versus emergent HD initiation in a tertiary-care setting.
Materials and Methods: This retrospective cohort study included adults with stage 5 chronic kidney disease who initiated HD at Siriraj Hospital between 2013 and 2022. Emergent initiation was defined as HD started for urgent indications without permanent vascular access, elective initiation was nephrologist-scheduled HD without acute complications. The primary outcomes were two-year all-cause mortality, cardiovascular events, hospitalizations, and vascular-access complications.
Results: Among 240 patients, 104 (43.3%) initiated HD emergently. These patients had higher rates of diabetes, poorer nutritional and metabolic profiles, less pre-dialysis care, and greater catheter use. Crude mortality was higher in the emergent group (15.4% vs. 10.3%), but after adjustment for comorbidities, functional status, and laboratory parameters, emergent initiation was not independently associated with mortality (adjusted HR 1.42, 95% CI 0.61–3.29). Infection-related deaths and vascular access infections were more frequent with emergent initiation, while vascular access dysfunction occurred more often in the elective group. Median hospitalization-free survival was shorter in the emergent group.
Conclusion: Emergent HD initiation was not an independent predictor of mortality, suggesting that excess risk observed in prior cohorts may reflect comorbidity and nutritional status rather than initiation type itself. Nevertheless, emergent initiation remained a marker of suboptimal pre-dialysis care and higher infection risk. Strengthening early nephrology referral, structured pre-dialysis planning, and infection prevention remains essential for optimizing ESRD outcomes.
References
Ingsathit A, Thakkinstian A, Chaiprasert A, Sangthawan P, Gojaseni P, Kiattisunthorn K, et al. Prevalence and risk factors of chronic kidney disease in the Thai adult population: Thai SEEK study. Nephrol Dial Transplant. 2010;25(5):1567-75.
Ong-Ajyooth L, Vareesangthip K, Khonputsa P, Aekplakorn W. Prevalence of chronic kidney disease in Thai adults: a national health survey. BMC Nephrol. 2009;10:35.
Perkovic V, Cass A, Patel AA, Suriyawongpaisal P, Barzi F, Chadban S, et al. High prevalence of chronic kidney disease in Thailand. Kidney Int. 2008;73(4):473-9.
Thai Renal Replacement Therapy (TRT) Registry 2023 Annual Data Report: The Subcommittee of the Thai Renal Replacement Therapy (TRT) Registry 2024, The Nephrology Society of Thailand; March 2025 [cited 2025 Apr 21]. Available from: https://www.nephrothai.org/wp-content/uploads/2025/03/Ebook-TRT-book-2023-10-Mar-2025Final.pdf.
Alnaser RI, Abed MN, Alassaf FA, Alsaaty MH. Integrating Artificial Intelligence into Chronic Kidney Disease Care: Enhancing Hemodialysis Scheduling, Comorbidity Management, and Diagnostic Capabilities. Siriraj Med J. 2025;77(7):543-52.
Mori K, Nishide K, Okuno S, Shoji T, Emoto M, Tsuda A, et al. Impact of diabetes on sarcopenia and mortality in patients undergoing hemodialysis. BMC Nephrol. 2019;20(1):105.
Couchoud C, Moranne O, Frimat L, Labeeuw M, Allot V, Stengel B. Associations between comorbidities, treatment choice and outcome in the elderly with end-stage renal disease. Nephrol Dial Transplant. 2007;22(11):3246-54.
Anutrakulchai S, Mairiang P, Pongskul C, Thepsuthammarat K, Chan-On C, Thinkhamrop B. Mortality and treatment costs of hospitalized chronic kidney disease patients between the three major health insurance schemes in Thailand. BMC Health Serv Res. 2016;16(1):528.
Michel A, Pladys A, Bayat S, Couchoud C, Hannedouche T, Vigneau C. Deleterious effects of dialysis emergency start, insights from the French REIN registry. BMC Nephrol. 2018;19(1):233.
Chen YM, Wang YC, Hwang SJ, Lin SH, Wu KD. Patterns of Dialysis Initiation Affect Outcomes of Incident Hemodialysis Patients. Nephron. 2016;132(1):33-42.
Stack AG. Impact of timing of nephrology referral and pre-ESRD care on mortality risk among new ESRD patients in the United States. Am J Kidney Dis. 2003;41(2):310-8.
Hwang SJ, Yang WC, Lin MY, Mau LW, Chen HC, Taiwan Society of N. Impact of the clinical conditions at dialysis initiation on mortality in incident haemodialysis patients: a national cohort study in Taiwan. Nephrol Dial Transplant. 2010;25(8):2616-24.
Wu LC, Lin MY, Hsieh CC, Chiu HC, Mau LW, Chiu YW, et al. Planned creation of vascular access saves medical expenses for incident dialysis patients. Kaohsiung J Med Sci. 2009;25(10):521-9.
Ethier J, Mendelssohn DC, Elder SJ, Hasegawa T, Akizawa T, Akiba T, et al. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant. 2008;23(10):3219-26.
Kazmi WH, Obrador GT, Khan SS, Pereira BJ, Kausz AT. Late nephrology referral and mortality among patients with end-stage renal disease: a propensity score analysis. Nephrol Dial Transplant. 2004;19(7):1808-14.
Pena JM, Logrono JM, Pernaute R, Laviades C, Virto R, Vicente de Vera C. Late nephrology referral influences on morbidity and mortality of hemodialysis patients. A provincial study. Nefrologia. 2006;26(1):84-97.
Gallego E, Lopez A, Lorenzo I, Lopez E, Llamas F, Illescas ML, et al. Influence of early or late referral to nephrologist over morbidity and mortality in hemodialysis. Nefrologia. 2003;23(3):234-42.
Diegoli H, Silva MC, Machado DS, Cruz CE. Late nephrologist referral and mortality association in dialytic patients. J Bras Nefrol. 2015;37(1):32-7.
Cheng L, Hu N, Song D, Liu L, Chen Y. Early versus late nephrology referral and patient outcomes in chronic kidney disease: an updated systematic review and meta-analysis. BMC Nephrol. 2025;26(1):25.
Watcharotone N, Moolvong P, Matula K, Kosukhvivadhana D. Survival outcome after decision making for renal replacement therapy in chronic renal failure. Journal of the Nephrology Society of Thailand. 2022;28(1):68-76.
Shimizu Y, Nakata J, Yanagisawa N, Shirotani Y, Fukuzaki H, Nohara N, et al. Emergent initiation of dialysis is related to an increase in both mortality and medical costs. Sci Rep. 2020;10(1):19638.
Wara-aswapati S, Chuasuwan A. Survival rate and associated factors of unplanned hemodialysis initiation among end stage kidney disease patients. Royal Thai Air Force Medical Gazette. 2022;68(1):10-20.
Vareesangthip K, Davenport A. Reducing the risk of intradialytic hypotension by altering the composition of the dialysate. Hemodial Int. 2020;24(3):276-81.
Vareesangthip K, Yincharoen P, Winijkul A, Chanchairujira T. Cardiac arrhythmia during early-week and mid-week dialysis in hemodialysis patients. Ther Apher Dial. 2021;25(6):890-8.
Srisuwan W, Charoensri S, Jantarakana K, Chanchairujira T. Increasing Dialysate Flow Rate over 500 ml/min for Reused High-Flux Dialyzers do not Increase Delivered Dialysis Dose: A Prospective Randomized Cross Over Study. Siriraj Med J. 2022;74(3):152-60.
Vareesangthip K, Thanapattaraborisuth B, Chanchairujira K, Wonglaksanapimon S, Chanchairujira T. Assessment of Volume Status in Chronic Hemodialysis: Comparison of Lung Ultrasound to Clinical Practice and Bioimpedance. Siriraj Med J. 2023;75(3):224-33.
Taesilapasathit C, Spanuchart I, Suppadungsuk S, Sutharattanapong N, Vipattawat K, Sethakarun S, et al. Accumulation of Advanced Glycation End Products Independently Increases the Risk of Hospitalization Among Hemodialysis Patients. Siriraj Med J. 2022;74(5):305-13.
Thaweethamcharoen T, Vasuvattakul S, Noparatayaporn P. Comparison of Utility Scores and Quality of Life Scores in Thai Patients between Twice and Thrice-Weekly Hemodialysis. Siriraj Med J. 2020;64(3):94-7.
Tangwonglert T, Vareesangthip K, Vongsanim S, Davenport A. Comparison of skin autofluorescence, a marker of tissue advanced glycation end-products in the fistula and non-fistula arms of patients treated by hemodialysis. Artif Organs. 2020;44(11):1224-7.
Mohamed H, Ali A, Browne LD, O'Connell NH, Casserly L, Stack AG, et al. Determinants and outcomes of access-related blood-stream infections among Irish haemodialysis patients; a cohort study. BMC Nephrol. 2019;20(1):68.
Campos E, Cuevas-Budhart MA, Cedillo-Flores R, Candelario-Lopez J, Jimenez R, Flores-Almonte A, et al. Is central venous catheter in haemodialysis still the main factor of mortality after hospitalization? BMC Nephrol. 2024;25(1):90.
Chaivanit T, Chaivanit P, Bumrungrachapukdee P, Unprasert P, Wattanavaekin K, Benyakorn T. Comparison of Primary Patency Rate between Drug- Coated Balloon and Plain Balloon Angioplasty in Hemodialysis Access. Siriraj Med J. 2022;74(6):388-94.
Additional Files
Published
How to Cite
License
Copyright (c) 2025 Siriraj Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Authors who publish with this journal agree to the following conditions:
Copyright Transfer
In submitting a manuscript, the authors acknowledge that the work will become the copyrighted property of Siriraj Medical Journal upon publication.
License
Articles are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0). This license allows for the sharing of the work for non-commercial purposes with proper attribution to the authors and the journal. However, it does not permit modifications or the creation of derivative works.
Sharing and Access
Authors are encouraged to share their article on their personal or institutional websites and through other non-commercial platforms. Doing so can increase readership and citations.









